23. Reproductive Freedom
|
Reproductive Freedom, or the rights to control your reproduction, came under attack by laws in the late 19th century. As soon as women gained political freedoms, they began attacking these restrictions in the 20th century, with advocacy efforts peaking in the 1960s. Rights to privacy, rights to contraception (birth control), and rights to abortion were all focal points for women and their allies.
Trigger warning: this section discusses rape and abortion. |
After women won the vote, many battles for women’s rights remained–especially in the area of reproductive rights which uniquely affected women, and had yet to be addressed by either Congress or almost all-male state legislatures.
While reproduction may seem awkward to talk about, it has been one of the most significant and defining facets of women’s lives throughout history. In the 20th century women pushed back against the laws of the late 19th century to expand their options and choices related to having children. This included birth control, access to abortion, maternity leave and child care. All of these efforts expanded women’s ability to join the workforce in greater numbers, but it was an uphill battle that took decades. Women had to fight against social norms, expected gender roles, and stigmas to redefine womanhood and femininity, to get a seat at the table where decisions were being made.
Forewarning, this section is going to discuss some difficult topics including rape, abortion, illegal abortion, and fetal abnormalities.
While reproduction may seem awkward to talk about, it has been one of the most significant and defining facets of women’s lives throughout history. In the 20th century women pushed back against the laws of the late 19th century to expand their options and choices related to having children. This included birth control, access to abortion, maternity leave and child care. All of these efforts expanded women’s ability to join the workforce in greater numbers, but it was an uphill battle that took decades. Women had to fight against social norms, expected gender roles, and stigmas to redefine womanhood and femininity, to get a seat at the table where decisions were being made.
Forewarning, this section is going to discuss some difficult topics including rape, abortion, illegal abortion, and fetal abnormalities.
 19th Century Male Doctor, Public Domain
19th Century Male Doctor, Public Domain
Background:
Because of the way society is structured, and because most laws are written to protect lawmakers’ interests, few laws protected women and mothers. In marriage, women had some protections under laws that ensured the father would provide for his children, but outside of marriage women had little options. It wasn’t until 1950 that Wisconsin became the first state to enact a formal child support law, which required fathers to provide financial support for their children. Even today, while child support laws are common, fathers are not required to provide support for pregnant mothers or help with hospital bills. Following Wisconsin, other states gradually implemented their own child support laws, but since this was before reliable paternity tests, it was difficult to prove men were in fact the father.
The Patriarchal system, a system in which elite men hold the power and poor men and most women are largely excluded from it, caused married women to almost disappear in marriage. Married women could not open bank accounts without their husbands signature until 1974 and women were listed not by their own name, but as their husband’s wife, on their passports. In the workforce, women still made fractions of what men made and there were little-to-no protections for women if they got pregnant. Men on the other hand could have sex, not acknowledge the pregnancy, support the woman during the pregnancy and birth, and fail to provide for the child on the other end, leaving the risks and expense of childbirth and childrearing on women.
Divorce was often harder for women to acquire. Established laws gave men more choice over when they could divorce, and traditionally, women financially relied on men for support, so divorce was often detrimental to a woman’s financial situation. Common reasons for divorce included adultery, abandonment, and cruelty, but proving these grounds was often challenging for women. Additionally, divorce proceedings could be costly, time-consuming, and required significant evidence and witnesses. Some states introduced laws that allowed women to petition for divorce on grounds of desertion or extreme cruelty. However, even with these provisions, women often faced significant legal and societal obstacles when seeking divorce. Furthermore, divorce often carried social stigmas and financial implications for women. In many cases, divorced women were at a disadvantage in terms of property rights, child custody, and financial support. It wasn’t until the 1970s that “no-fault divorce” became more common
These vestiges, or hold outs, from the 19th century made women dependant on men to provide for them and their children. Moral and social conventions dictated that women not engage in sex before marriage. Marriage provided a woman with financial stability–theoretically–and provided a man with social status and sexual access. Once in a marriage, however, there were few options for women to leave, there were repercussions for her socially and economically if she did. If a woman became pregnant out of wedlock–her refusal to adhere to social and moral conventions meant that the father of the child was not obligated to provide for her or their child. It all created a system and structure wherein women were punished or denied protections if they stepped out of line.
Women in this period worked to change the laws that would make them better able to provide for their children without men, but they also looked at the root cause of the problem: sex. If women could increase their control over when they got pregnant or if they carried their pregnancy to term, then they could be more equal in society. This concept of control over your body is called “Reproductive Freedom.” Reproductive Freedom can’t exist where a woman has no ability to control what happens to her body. This is deeply important, especially for women where pregnancy carries health risks like high blood pressure, preeclampsia, gestational diabetes, genetic birth defects, and more.
Those are the challenges faced by women who have consensual sex, meaning they agreed to have sex. There are sadly also cases where people are coerced and forced into sexual acts. This is called rape. In the early 20th century, especially for Black women, rape was common, because again, the entire social and legal landscape was built to protect men. Today, one in four women have experienced attempted or completed rape.
For women of color, sexual abuse was a holdover from the culture of slavery in the south. Enslaved women in the US were “owned” by men who claimed access to their bodies and to any children born of sexual encounters between master and slave. Enslaved mothers had no choice over whether they had sex with the master and no rights to her children after they were born. In the decades after slavery, the southern rape culture persisted.
Reproductive Freedom is important for women when all the scales of the system are tipped to favor men. It protects women and ensures their children are raised in supportive environments.
Women in Developmental Biology:
Many actors on both sides of the struggle for reproductive justice – politicians, activists and religious leaders – make scientific claims to justify their positions. Interestingly, the field of developmental biology (that is, the study of how animals and plants grow and develop) has been well-populated with women since WWII. Even before then it was Nettie Stevens (1861-1912) who identified how X and Y chromosomes were responsible for sex-determination by studying mealworms. In the 1920s and 1930s, women were also more represented in the field of embryology (the study of embryos) for a number of potential reasons: it often involved slow-moving fieldwork over several years that appealed less to publication-oriented male professional and it involved a high degree of fine motor skills that were encouraged in women doing needlework.
The founder of developmental genetics, Salome Gluecksohn-Waelsch was born in Danzig, Germany in 1907 and earned her doctorate from the University of Freiburg in 1932–studying the development of salamander embryos. In 1933, she and her husband escaped Nazi Germany for New York City. She was just one of hundreds of Jewish scientists to flee Germany on the eve of WWII. In America she joined Columbia University as a “research associate.” In that role she was able to publish a number of papers that made clear the connection between genetics and embryo development, a novel contribution that established the field of developmental genetics.
These scientists worked together to promote the cause of fellow women scientists. Jane Marion Oppenheimer (1911-1996) was a friend of Waelsch and a professor of biology and the history of science at Bryn Mawr College. She was an embryologist whose experimental work focused on the embryo of the common minnow. In addition to her own rich career on regulation and differentiation in embryos, Oppenheimer supported her colleague by singing the praises of Waelsch’s work to Ernst Scharrer, who was hiring for the newly founded Albert Einstein College of Medicine in New York. He ended up hiring Waelsch, finally giving her a full faculty position.
However, the most famous embryologist is probably Christiane Nüsslein-Volhard, who won the 1995 Nobel Prize in Physiology or Medicine for her work on how the genes in a fertilized egg form an embryo. Born in Germany in the middle of WWII, she studied biology, physics, and biochemistry, eventually earning her Ph.D. through her dissertation work on genetics. She became interested in how genes controlled the development of embryos. She and her colleague, Eric Wieschaus, worked with fruit flies and determined how the shape of fly embryos was determined by a small number of genes. While these women have worked to unlock the mysteries of how life is formed and developed, they can shed little light on the moral questions that are debated around reproductive rights. Those discussions take place not in the lab, but in households and the halls of power.
Because of the way society is structured, and because most laws are written to protect lawmakers’ interests, few laws protected women and mothers. In marriage, women had some protections under laws that ensured the father would provide for his children, but outside of marriage women had little options. It wasn’t until 1950 that Wisconsin became the first state to enact a formal child support law, which required fathers to provide financial support for their children. Even today, while child support laws are common, fathers are not required to provide support for pregnant mothers or help with hospital bills. Following Wisconsin, other states gradually implemented their own child support laws, but since this was before reliable paternity tests, it was difficult to prove men were in fact the father.
The Patriarchal system, a system in which elite men hold the power and poor men and most women are largely excluded from it, caused married women to almost disappear in marriage. Married women could not open bank accounts without their husbands signature until 1974 and women were listed not by their own name, but as their husband’s wife, on their passports. In the workforce, women still made fractions of what men made and there were little-to-no protections for women if they got pregnant. Men on the other hand could have sex, not acknowledge the pregnancy, support the woman during the pregnancy and birth, and fail to provide for the child on the other end, leaving the risks and expense of childbirth and childrearing on women.
Divorce was often harder for women to acquire. Established laws gave men more choice over when they could divorce, and traditionally, women financially relied on men for support, so divorce was often detrimental to a woman’s financial situation. Common reasons for divorce included adultery, abandonment, and cruelty, but proving these grounds was often challenging for women. Additionally, divorce proceedings could be costly, time-consuming, and required significant evidence and witnesses. Some states introduced laws that allowed women to petition for divorce on grounds of desertion or extreme cruelty. However, even with these provisions, women often faced significant legal and societal obstacles when seeking divorce. Furthermore, divorce often carried social stigmas and financial implications for women. In many cases, divorced women were at a disadvantage in terms of property rights, child custody, and financial support. It wasn’t until the 1970s that “no-fault divorce” became more common
These vestiges, or hold outs, from the 19th century made women dependant on men to provide for them and their children. Moral and social conventions dictated that women not engage in sex before marriage. Marriage provided a woman with financial stability–theoretically–and provided a man with social status and sexual access. Once in a marriage, however, there were few options for women to leave, there were repercussions for her socially and economically if she did. If a woman became pregnant out of wedlock–her refusal to adhere to social and moral conventions meant that the father of the child was not obligated to provide for her or their child. It all created a system and structure wherein women were punished or denied protections if they stepped out of line.
Women in this period worked to change the laws that would make them better able to provide for their children without men, but they also looked at the root cause of the problem: sex. If women could increase their control over when they got pregnant or if they carried their pregnancy to term, then they could be more equal in society. This concept of control over your body is called “Reproductive Freedom.” Reproductive Freedom can’t exist where a woman has no ability to control what happens to her body. This is deeply important, especially for women where pregnancy carries health risks like high blood pressure, preeclampsia, gestational diabetes, genetic birth defects, and more.
Those are the challenges faced by women who have consensual sex, meaning they agreed to have sex. There are sadly also cases where people are coerced and forced into sexual acts. This is called rape. In the early 20th century, especially for Black women, rape was common, because again, the entire social and legal landscape was built to protect men. Today, one in four women have experienced attempted or completed rape.
For women of color, sexual abuse was a holdover from the culture of slavery in the south. Enslaved women in the US were “owned” by men who claimed access to their bodies and to any children born of sexual encounters between master and slave. Enslaved mothers had no choice over whether they had sex with the master and no rights to her children after they were born. In the decades after slavery, the southern rape culture persisted.
Reproductive Freedom is important for women when all the scales of the system are tipped to favor men. It protects women and ensures their children are raised in supportive environments.
Women in Developmental Biology:
Many actors on both sides of the struggle for reproductive justice – politicians, activists and religious leaders – make scientific claims to justify their positions. Interestingly, the field of developmental biology (that is, the study of how animals and plants grow and develop) has been well-populated with women since WWII. Even before then it was Nettie Stevens (1861-1912) who identified how X and Y chromosomes were responsible for sex-determination by studying mealworms. In the 1920s and 1930s, women were also more represented in the field of embryology (the study of embryos) for a number of potential reasons: it often involved slow-moving fieldwork over several years that appealed less to publication-oriented male professional and it involved a high degree of fine motor skills that were encouraged in women doing needlework.
The founder of developmental genetics, Salome Gluecksohn-Waelsch was born in Danzig, Germany in 1907 and earned her doctorate from the University of Freiburg in 1932–studying the development of salamander embryos. In 1933, she and her husband escaped Nazi Germany for New York City. She was just one of hundreds of Jewish scientists to flee Germany on the eve of WWII. In America she joined Columbia University as a “research associate.” In that role she was able to publish a number of papers that made clear the connection between genetics and embryo development, a novel contribution that established the field of developmental genetics.
These scientists worked together to promote the cause of fellow women scientists. Jane Marion Oppenheimer (1911-1996) was a friend of Waelsch and a professor of biology and the history of science at Bryn Mawr College. She was an embryologist whose experimental work focused on the embryo of the common minnow. In addition to her own rich career on regulation and differentiation in embryos, Oppenheimer supported her colleague by singing the praises of Waelsch’s work to Ernst Scharrer, who was hiring for the newly founded Albert Einstein College of Medicine in New York. He ended up hiring Waelsch, finally giving her a full faculty position.
However, the most famous embryologist is probably Christiane Nüsslein-Volhard, who won the 1995 Nobel Prize in Physiology or Medicine for her work on how the genes in a fertilized egg form an embryo. Born in Germany in the middle of WWII, she studied biology, physics, and biochemistry, eventually earning her Ph.D. through her dissertation work on genetics. She became interested in how genes controlled the development of embryos. She and her colleague, Eric Wieschaus, worked with fruit flies and determined how the shape of fly embryos was determined by a small number of genes. While these women have worked to unlock the mysteries of how life is formed and developed, they can shed little light on the moral questions that are debated around reproductive rights. Those discussions take place not in the lab, but in households and the halls of power.
 Anthony Comstock, Public Domain
Anthony Comstock, Public Domain
Comstock Laws:
So what does Reproductive Freedom look like? Most advocates agree that it includes things like the freedom to have sex or not when one chooses, the freedom to contraception (birth control) and access to it, the right to abortion and access to it, the right to parental leave to keep your job while you birth and raise an infant in its early months, access to affordable childcare, and tax breaks for single parents among other things. These of course were the battles fought during the late 19th century and through today.
The biggest barrier to women’s reproductive freedoms were laws passed by men in the 19th century. It’s important to note that these laws were not in practice during the founding of the US, but added later. The laws started with the formation of the American Medical Association (AMA) in 1847. Male doctors banded together to delegitimize the mostly female midwives who were competing for services with them. Over time, the midwives’ practices disappeared in favor of male doctors. Despite having little experience or exposure to pregnancy and birth practices, these doctors assumed that their medical degrees afforded them greater expertise in the field of women’s health and childbirth.
The most important of these oppressive laws were the Comstock Laws. The Comstock Laws were a series of federal acts in the late 19th and early 20th centuries. These laws were named after their chief architect, Anthony Comstock, a zealous advocate against what he saw as “vices.” Comstock succeeded in passing the first of these laws in 1873. They were designed to prohibit and regulate the distribution of materials deemed to be obscene, immoral, or indecent, particularly related to contraception and information about birth control. Birth control is a broad term used to describe devices or chemicals that could help prevent pregnancy. They include all forms of condoms, hormones, implantable devices in the vagina, and sterilization. People like Comstock believed that birth control would cause people to have riskier sex because the threat of pregnancy would be removed. Many religious people also believed that sex should be reserved solely for the purpose of reproduction.
Under the Comstock Laws, it was illegal to send through the mail any materials, including books, pamphlets, and contraceptives, that were considered obscene or lewd. The laws also targeted the distribution of information about abortion and contraception, making it punishable by imprisonment or fines.
Because men were the doctors, the lawyers, and the government officials, women had little say in the passage of these laws. Even today women make up a small minority in all of those professions.
Women of the late 19th century didn’t take these laws sitting down. Emma Goldman, for example, was an influential political activist and writer, born in 1869 in the Russian Empire (now Lithuania) and later emigrated to the United States. She played a prominent role in various social and political movements, advocating for women's rights, workers' rights, free speech, and anarchism.
So what does Reproductive Freedom look like? Most advocates agree that it includes things like the freedom to have sex or not when one chooses, the freedom to contraception (birth control) and access to it, the right to abortion and access to it, the right to parental leave to keep your job while you birth and raise an infant in its early months, access to affordable childcare, and tax breaks for single parents among other things. These of course were the battles fought during the late 19th century and through today.
The biggest barrier to women’s reproductive freedoms were laws passed by men in the 19th century. It’s important to note that these laws were not in practice during the founding of the US, but added later. The laws started with the formation of the American Medical Association (AMA) in 1847. Male doctors banded together to delegitimize the mostly female midwives who were competing for services with them. Over time, the midwives’ practices disappeared in favor of male doctors. Despite having little experience or exposure to pregnancy and birth practices, these doctors assumed that their medical degrees afforded them greater expertise in the field of women’s health and childbirth.
The most important of these oppressive laws were the Comstock Laws. The Comstock Laws were a series of federal acts in the late 19th and early 20th centuries. These laws were named after their chief architect, Anthony Comstock, a zealous advocate against what he saw as “vices.” Comstock succeeded in passing the first of these laws in 1873. They were designed to prohibit and regulate the distribution of materials deemed to be obscene, immoral, or indecent, particularly related to contraception and information about birth control. Birth control is a broad term used to describe devices or chemicals that could help prevent pregnancy. They include all forms of condoms, hormones, implantable devices in the vagina, and sterilization. People like Comstock believed that birth control would cause people to have riskier sex because the threat of pregnancy would be removed. Many religious people also believed that sex should be reserved solely for the purpose of reproduction.
Under the Comstock Laws, it was illegal to send through the mail any materials, including books, pamphlets, and contraceptives, that were considered obscene or lewd. The laws also targeted the distribution of information about abortion and contraception, making it punishable by imprisonment or fines.
Because men were the doctors, the lawyers, and the government officials, women had little say in the passage of these laws. Even today women make up a small minority in all of those professions.
Women of the late 19th century didn’t take these laws sitting down. Emma Goldman, for example, was an influential political activist and writer, born in 1869 in the Russian Empire (now Lithuania) and later emigrated to the United States. She played a prominent role in various social and political movements, advocating for women's rights, workers' rights, free speech, and anarchism.
 Margaret Sanger, Public Domain
Margaret Sanger, Public Domain
Margaret Sanger:
Perhaps the most well-known advocate of birth control was Margaret Sanger, the founder of Planned Parenthood. When Margaret Sanger opened her clinic on Manhattan’s Lower East Side in 1916, immigrant women from Eastern and Southern Europe, the majority of whom were Catholic or Orthodox Jewish, flocked to her for help. Her goal was to distribute information on contraception in order to help women plan the birth of their children and avoid dangerous “back alley abortions” that frequently caused death. Sanger was arrested and tried under New York’‘s Comstock Laws for informing women about methods of contraception.
Prior to Sanger’s crusade for safe contraception, doctors had little advice to offer to women who wished to avoid pregnancy. One woman told Sanger that her doctor had only advised her to tell her husband to “sleep on the roof” in order to avoid sex altogether. Clearly, such advice did not provide effective birth control, and was meaningless in a society where women were unable to deny their husband’s sexual advances.
Sanger founded the American Birth Control League in 1921 to promote her pro-contraception philosophy.This organization was the precursor of The Planned Parenthood Federation of
America , an organization that fights for reproductive freedom for all people.
Sanger’s unfortunate advocacy of Eugenics as a means of controlling population tarnished her reputation. Eugenics was a science that promoted the idea of “better breeding;” however, the means through which this was accomplished was often through the sterilizing, or making it impossible for them to have children, of undesirable portions of the population, typically racial and religious minorities. The theory used Darwinism to suggest that a population could be “strengthened” by inhibiting the reproduction of its “weakest” people. Eugenics was widespread in the US and western Europe and was foundational to Nazi ideology leading up to World War II. Because of the Nazi’s application of Eugenics to justify exterminating the Jewish population, Eugenics was discredited as pseudoscience that disguised racism.
Margarett Sanger and others shifted away from Eugenics to support “family planning,” which instead of stopping certain populations from having children, gave them options and support to control when they had children. Elements of eugenicist thinking survived in the US, but the legal and political emphasis shifted to providing significant support for the poorest in American society. One part of that assistance was information on family planning so that families could devote their resources to supporting their living children.
Perhaps the most well-known advocate of birth control was Margaret Sanger, the founder of Planned Parenthood. When Margaret Sanger opened her clinic on Manhattan’s Lower East Side in 1916, immigrant women from Eastern and Southern Europe, the majority of whom were Catholic or Orthodox Jewish, flocked to her for help. Her goal was to distribute information on contraception in order to help women plan the birth of their children and avoid dangerous “back alley abortions” that frequently caused death. Sanger was arrested and tried under New York’‘s Comstock Laws for informing women about methods of contraception.
Prior to Sanger’s crusade for safe contraception, doctors had little advice to offer to women who wished to avoid pregnancy. One woman told Sanger that her doctor had only advised her to tell her husband to “sleep on the roof” in order to avoid sex altogether. Clearly, such advice did not provide effective birth control, and was meaningless in a society where women were unable to deny their husband’s sexual advances.
Sanger founded the American Birth Control League in 1921 to promote her pro-contraception philosophy.This organization was the precursor of The Planned Parenthood Federation of
America , an organization that fights for reproductive freedom for all people.
Sanger’s unfortunate advocacy of Eugenics as a means of controlling population tarnished her reputation. Eugenics was a science that promoted the idea of “better breeding;” however, the means through which this was accomplished was often through the sterilizing, or making it impossible for them to have children, of undesirable portions of the population, typically racial and religious minorities. The theory used Darwinism to suggest that a population could be “strengthened” by inhibiting the reproduction of its “weakest” people. Eugenics was widespread in the US and western Europe and was foundational to Nazi ideology leading up to World War II. Because of the Nazi’s application of Eugenics to justify exterminating the Jewish population, Eugenics was discredited as pseudoscience that disguised racism.
Margarett Sanger and others shifted away from Eugenics to support “family planning,” which instead of stopping certain populations from having children, gave them options and support to control when they had children. Elements of eugenicist thinking survived in the US, but the legal and political emphasis shifted to providing significant support for the poorest in American society. One part of that assistance was information on family planning so that families could devote their resources to supporting their living children.
 Katharine Dexter McCormick, Wikimedia Commons
Katharine Dexter McCormick, Wikimedia Commons
The Pill:
Then in the late 1950s early 1960s a scientific revolution made contraceptives easier and more effective. As early as the 1940s, Margaret Sanger, as president of Planned Parenthood, closely monitored and funded birth control research. Sanger's friend, Katharine Dexter McCormick, generously funded research for an oral contraceptive, which people theorized would be more effective. McCormick was a women's rights advocate and a graduate of MIT. She contributed to the suffrage movement and League of Women Voters. After her husband's passing, she pledged $10,000 and later provided annual contributions exceeding $150,000 annually for contraceptive research.
The development of the oral contraceptive relied on ancient Aztec medical traditions. Russell Marker discovered the contraceptive properties of the Barbasco root, from which progestin was extracted and combined with estrogen by Gregory Pincus to create the first pill. McCormick funded initial clinical trials conducted by Dr. John Rock, a renowned gynecologist and devout Catholic. Rock's book advocating for the acceptance of the oral contraceptive by the Catholic Church was unsuccessful.
Due to Massachusetts' restrictive laws, Rock chose Puerto Rico for trials, where contraception was legal, birth control clinics existed, and trusted US-trained medical practitioners were present. Puerto Rican women desired effective birth control. The trials required specific criteria for participation, and they began in April 1956 with ongoing successes reported. The FDA approved the pill for menstrual regulation in 1957 and for sale in 1960. While this was an important milestone, it is important to recognize that these trials in Puerto Rico were also somewhat problematic. As testing evolved from things like sperimicides and jellies–which are far less effective–some scientists ascribed their lower success rates to Puerto Rican women’s presumed fecundity, hypersexuality, and lower intelligence rates. Though many Puerto Rican wanted access to birth control, this also put them in direct contact with white American scientists who came to Puerto Rico with their own existing racial ideologies that were informed by decades of US imperialism on the island. As such, Puerto Rico also became a site where abuses ran rampant–by the 1980s, it was discovered that more than ⅓ of Puerto Rican women had been coerced into sterilization procedures–la operación–or permanent birth control.
Enovid, the first oral contraceptive, gained popularity, with one in four married women under 45 using it by 1965. Sanger's efforts established family planning as the norm, significantly reducing unintended pregnancies. The first pill had higher hormone levels than necessary, unlike current lower-dose pills and thus had lots of side effects. It took time for doctors to figure out the root issues, and scientists to figure out the lowest effective dosages.
Then in the late 1950s early 1960s a scientific revolution made contraceptives easier and more effective. As early as the 1940s, Margaret Sanger, as president of Planned Parenthood, closely monitored and funded birth control research. Sanger's friend, Katharine Dexter McCormick, generously funded research for an oral contraceptive, which people theorized would be more effective. McCormick was a women's rights advocate and a graduate of MIT. She contributed to the suffrage movement and League of Women Voters. After her husband's passing, she pledged $10,000 and later provided annual contributions exceeding $150,000 annually for contraceptive research.
The development of the oral contraceptive relied on ancient Aztec medical traditions. Russell Marker discovered the contraceptive properties of the Barbasco root, from which progestin was extracted and combined with estrogen by Gregory Pincus to create the first pill. McCormick funded initial clinical trials conducted by Dr. John Rock, a renowned gynecologist and devout Catholic. Rock's book advocating for the acceptance of the oral contraceptive by the Catholic Church was unsuccessful.
Due to Massachusetts' restrictive laws, Rock chose Puerto Rico for trials, where contraception was legal, birth control clinics existed, and trusted US-trained medical practitioners were present. Puerto Rican women desired effective birth control. The trials required specific criteria for participation, and they began in April 1956 with ongoing successes reported. The FDA approved the pill for menstrual regulation in 1957 and for sale in 1960. While this was an important milestone, it is important to recognize that these trials in Puerto Rico were also somewhat problematic. As testing evolved from things like sperimicides and jellies–which are far less effective–some scientists ascribed their lower success rates to Puerto Rican women’s presumed fecundity, hypersexuality, and lower intelligence rates. Though many Puerto Rican wanted access to birth control, this also put them in direct contact with white American scientists who came to Puerto Rico with their own existing racial ideologies that were informed by decades of US imperialism on the island. As such, Puerto Rico also became a site where abuses ran rampant–by the 1980s, it was discovered that more than ⅓ of Puerto Rican women had been coerced into sterilization procedures–la operación–or permanent birth control.
Enovid, the first oral contraceptive, gained popularity, with one in four married women under 45 using it by 1965. Sanger's efforts established family planning as the norm, significantly reducing unintended pregnancies. The first pill had higher hormone levels than necessary, unlike current lower-dose pills and thus had lots of side effects. It took time for doctors to figure out the root issues, and scientists to figure out the lowest effective dosages.
 Estelle Griswold, Public Domain
Estelle Griswold, Public Domain
Griswold v. Connecticut:
Finally, that same year, 1965 the Supreme Court ruled in Griswold v. Connecticut that married couples had a right to utilize birth control methods based on the right to privacy that is suggested but not explicitly defined in the 14th Amendment of the US Constitution. The plaintiffs were Estelle Griswold, who was the executive director of the Planned Parenthood League of Connecticut at the time, and Dr. C. Lee Buxton, who was a physician and a professor at the Yale School of Medicine. They challenged the constitutionality of a Connecticut law that criminalized the use of contraceptives, even by married couples.
Estelle Griswold and Dr. Buxton were arrested and convicted for providing contraceptive advice and services to married individuals. They argued that the Connecticut law violated the right to privacy and interfered with the intimate decisions made by married couples regarding family planning. This case was landmark and led to other cases that expanded reproductive freedoms to unmarried couples, like Eisenstadt v. Baird.
Finally, that same year, 1965 the Supreme Court ruled in Griswold v. Connecticut that married couples had a right to utilize birth control methods based on the right to privacy that is suggested but not explicitly defined in the 14th Amendment of the US Constitution. The plaintiffs were Estelle Griswold, who was the executive director of the Planned Parenthood League of Connecticut at the time, and Dr. C. Lee Buxton, who was a physician and a professor at the Yale School of Medicine. They challenged the constitutionality of a Connecticut law that criminalized the use of contraceptives, even by married couples.
Estelle Griswold and Dr. Buxton were arrested and convicted for providing contraceptive advice and services to married individuals. They argued that the Connecticut law violated the right to privacy and interfered with the intimate decisions made by married couples regarding family planning. This case was landmark and led to other cases that expanded reproductive freedoms to unmarried couples, like Eisenstadt v. Baird.
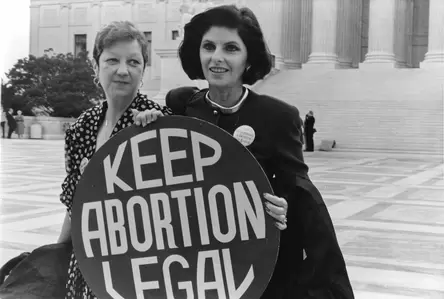 Norma McCorvey and her attorney, Wikimedia Commons
Norma McCorvey and her attorney, Wikimedia Commons
Roe v. Wade:
Reproductive freedom isn’t just about preventing pregnancy, it’s about the freedom to decide what happens to one’s body, control your financial future, and make the choice to be a mom. Some people have argued that consenting to sex is tacit consent to be a mother, but the long history of the patriarchy shows that the same or tacit consent has not fallen equally on men with fatherhood. Therefore some feminists argue that this argument is rooted in misogyn and a sexual double standard for women.
Abortion is a broad medical term that refers to termination of a pregnancy. It includes spontaneous abortions and induced abortions. Spontaneous abortions are often euphemistically referred to as “miscarriages;” however, in professional medical parlance (like the GTPAL acronym that defines a women’s reproductive medical history), the term is abortion. Induced abortions are what we socially think of as “abortion.”
When it comes to induced abortions, they can be performed at any stage of a pregnancy; however, according to data from 2020, 93% of abortions happen before 13-weeks gestation (within the first trimester). This is before the mother is noticeably pregnant, before the fetus can be felt moving around, and before fetal viability. Abortions before nine weeks are typically done using medications that block hormone signals to the pregnancy and cause the uterus to contract and expel the embryo, a term for the cells that eventually become a fetus at 9 weeks.
Statistically few abortions occur in the second and third trimesters. 5.8% of abortions occur between 14 and 20 weeks of pregnancy, which is in the second trimester. 20 weeks is around when fetal movement can be felt. Induced abortions that occur in the second and third trimester almost always are performed because of potential health risks to the pregnant woman or fetus. As it stands, most prenatal screenings for fetal diseases or defects cannot be performed until the second trimester–thus delaying when it is feasible for a woman who discovers her fetus carries some type of disease to acquire an abortion. Less than 1% of abortions happen after 20 weeks and it is usually an extreme, health related circumstance. Abortions that happen after medication is effective are performed surgically and involve a doctor using tools to terminate the pregnancy.
In the politicized discussions around abortion, much has been made about the pain mothers and, or fetus’ feel during abortion. Studies have shown that for pregnant people, abortion is safer than carrying a pregnancy to term and birth. This was also true for most of US history. Pregnancy is not a health-neutral event and carries with it risks–including the risk of death. For the embryo or fetus, abortion ends the lifelike activity, but it is debated by professionals how painful this is and the evidence varies by when the abortion is performed. Public opinion polls have varied since the 1960s on abortion, most people agree it is ending life, but most also feel it’s different from ending the life of something that has been born.
Throughout the early 20th century women and their doctors were put on trial for violating state abortion laws. By 1910, abortion was illegal in every state in the US. Only some states had built in exceptions to save the mother’s life. The decision of when a mother’s life was in jeopardy was left to doctors, who were almost all men, and these standards were not universal.
Making abortion illegal, also known as criminalizing it, simply meant that more women turned away from qualified people to have abortions. Getting abortions under extreme circumstances by people willing to do something illegal, resulted in an increased death toll for mothers. Abortion was not inherently unsafe, illegal abortion was. In 1930, nearly 2,700 US women died from an illegal abortion, or one in five maternal deaths that year.
Doctors caught performing abortions were put on trial and lost their medical licenses. Increasingly the press covered stories about women who had died from an illegal abortion. Women’s bodies were found in barrels, chopped up in suitcases, all after a botched abortion by someone unqualified. People began calling for abortion law reform.
But more importantly, women began appearing in court to give testimony as to why they wanted one in the first place. Abortion was so stigmatized that women never talked about it. Stories of safe, successful abortions were never in the press; however, stories about illegal abortions that resulted in death sold papers. Thus, the effect of criminalization was that women who were accused were forced to talk about it publicly. Women who believed they would never get an abortion listened to abortion stories and empathized with the mothers choice, given her circumstances. Criminalization forced women to talk about their darkest moments in a very public forum.
In 1955, Planned Parenthood called for a national conference on abortion. The few doctors who attended called for greater flexibility for doctors to perform abortions. These doctors had personally witnessed women dying from pregnancy-related causes unable to help them, or watched women carry babies to term knowing the baby could not survive more than a week or so.
Then in the 1960s a drug often prescribed to women to treat pregnancy discomforts, like morning sickness, was found to cause birth defects in babies. A television personality, Sherri Chessen Finkbine was expecting her fifth child when she consumed tranquilizers that her husband brought from England to relieve her nausea, the drug thalidomide. However, after reading an article about thalidomide that discussed its role in the birth of thousands of babies born without arms or legs, Finkbine became worried about the potential harm to her unborn child. Finkbine's doctor confirmed her fears, but at the time, there was no test to assess the fetus's condition. So, following her doctor's suggestion, Finkbine and her husband decided to quietly have an abortion. Abortion in Arizona was illegal, so they ended up traveling to Sweden. Her case was public and public opinion polls showed that 52% of Americans supported her choice under the circumstances.
Ironically, the United States did not witness a pharmaceutical disaster on par with Europe related to Thalidomide because of one scientist at the Food and Drug Administration (FDA): Dr. Frances Kathleen Oldham Kelsey. Dr. Kelsey worked for the American Medical Association and eventually taught pharmacology at the University of South Dakota. In addition to her Ph.D., she also had her medical degree and briefly worked as general practitioner. It was in her first month in her position at the FDA that Dr. Kelsey was taked with evaluating the drug thalidomide for approval in the United States. When the manufacturers of thalidomide submitted their information to Dr. Kelsey, she didn’t believe they had provided adequate data to show its safety and asked them to resubmit their application once they had effectively proved its safety. The manufacturers were frustrated by this woman’s attempt to slow their approval process for a drug that was already in widespread use in Europe. Instead of conducting the new tests and submitting a new report, the manufacturers attempted to pressure and coerce Dr. Kelsey into approval. However, she held firm–trusting her extensive expertise. This back-and-forth is what ultimately caused enough of a delay for word to spread of fetal anomalies and defects in Europe related to thalidomide use by pregnant women. After a congressional hearing on the matter, Dr. Kelsey was able to ensure that thalidomide would be banned in the United States. In 1962, just a year later, President John F. Kennedy granted Dr. Kelsey the President's Award for Distinguished Federal Civilian Service. She was only the second woman to ever receive the award. Kennedy acknowledged "Her exceptional judgment in evaluating a new drug for safety for human use…” In the immediate aftermath of the thalidomide disaster, Dr. Kelsey helped change laws about drug approval to protect the patient, ensure informed consent in clinical trials, and reporting of adverse side effects to the FDA. In her long and distinguished career at the FDA, Dr. Kelsey would eventually become chief of the Division of New Drugs, director of the Division of Scientific Investigations, and deputy for Scientific and Medical Affairs in the Office of Compliance. She retired in 2005, at the age of 90, after 45 years of service.
Dr. Kelsey receiving the President’s Award for Distinguished Federal Civilian Service from President Kennedy. National Library of Medicine, Images from the History of Medicine.
While thousands of babies would be born with thalidomide-related deformities, the United States was spared from a tragedy of that scale. However, when combined with the realization that many of these women in Europe were married and otherwise respectable women and mothers, this public concern about disabled babies–in an era when disability was considered shameful–helped to open the door for discussions about elective abortion and relaxing existing abortion laws.
Despite the stereotype of the young, naive, and sexually promiscuous girl being the ones who get abortions, studies showed that women who were already mothers were more likely to get abortions and that religiosity was not a factor. Women of all faiths got abortions.
In 1964, abortion law reform activists registered their first national group: the Association for the Study of Abortion (ASA). Then in 1966, a group of nine highly regarded California doctors faced a lawsuit for providing abortions to women who had contracted rubella, a disease that could harm unborn babies. However, doctors from all over the country rallied to support these doctors, with even 128 medical school deans joining their defense. As a result, one of the earliest changes to abortion laws in the United States occurred. California revised its strict ban on abortion to permit hospital committees to review and approve requests for the procedure.
Studies in the 1960s showed that poor women and their families were affected to a greater extent from abortion bans. One study examined low-income women in New York City and found that 8% had tried to end a pregnancy through illegal means. Additionally, 38% reported that someone they knew had attempted to get an abortion. Among the low-income women who admitted having an abortion, 77% said they had attempted a self-induced procedure, while only a small fraction 2% involved a medical professional at all.
By the end of the 1960s there was a full fledged movement to repeal abortion bans. National Association for the Repeal of Abortion Laws (NARAL) was founded in 1969. NARAL became the first nationwide organization dedicated exclusively to advocating for the legalization of abortion. Left and right states were repealing or modifying their abortion stances. Alaska, Hawaii, New York, and Washington completely eliminated their laws prohibiting abortion, while 13 other states introduced changes that broadened the circumstances under which abortion was permitted. Instead of solely permitting abortion to save the life of the mother, these reforms allowed for abortion in situations where the pregnancy posed risks to the patient's physical or mental health, when there were fetal abnormalities, or when the pregnancy resulted from rape or incest. However, much of these changes were piecemeal and state by state. It would not be until 1973 that the question of abortion was answered federally.
The Roe v. Wade decision was a landmark ruling by the United States Supreme Court in 1973 that legalized abortion across the country. The case originated in Texas and involved a woman named Norma McCorvey, referred to as "Jane Roe" to protect her identity, who sought to terminate her pregnancy but was denied access to legal abortion under Texas law. In 1969, when McCorvey became pregnant, she was unmarried, financially struggling, and unable to afford to travel to a state where abortion was legal. This also wasn’t her first pregnancy. Texas law at the time prohibited abortion except to save the life of the mother or in instances of rape. McCorvey's lawyers, Linda Coffee and Sarah Weddington, sought a representative plaintiff who could best illustrate the difficulties faced by women seeking abortions. They aimed to demonstrate that the Texas law violated women's constitutional right to privacy. McCorvey's circumstances and her inability to access a safe and legal abortion made her a suitable candidate for the case.
Reproductive freedom isn’t just about preventing pregnancy, it’s about the freedom to decide what happens to one’s body, control your financial future, and make the choice to be a mom. Some people have argued that consenting to sex is tacit consent to be a mother, but the long history of the patriarchy shows that the same or tacit consent has not fallen equally on men with fatherhood. Therefore some feminists argue that this argument is rooted in misogyn and a sexual double standard for women.
Abortion is a broad medical term that refers to termination of a pregnancy. It includes spontaneous abortions and induced abortions. Spontaneous abortions are often euphemistically referred to as “miscarriages;” however, in professional medical parlance (like the GTPAL acronym that defines a women’s reproductive medical history), the term is abortion. Induced abortions are what we socially think of as “abortion.”
When it comes to induced abortions, they can be performed at any stage of a pregnancy; however, according to data from 2020, 93% of abortions happen before 13-weeks gestation (within the first trimester). This is before the mother is noticeably pregnant, before the fetus can be felt moving around, and before fetal viability. Abortions before nine weeks are typically done using medications that block hormone signals to the pregnancy and cause the uterus to contract and expel the embryo, a term for the cells that eventually become a fetus at 9 weeks.
Statistically few abortions occur in the second and third trimesters. 5.8% of abortions occur between 14 and 20 weeks of pregnancy, which is in the second trimester. 20 weeks is around when fetal movement can be felt. Induced abortions that occur in the second and third trimester almost always are performed because of potential health risks to the pregnant woman or fetus. As it stands, most prenatal screenings for fetal diseases or defects cannot be performed until the second trimester–thus delaying when it is feasible for a woman who discovers her fetus carries some type of disease to acquire an abortion. Less than 1% of abortions happen after 20 weeks and it is usually an extreme, health related circumstance. Abortions that happen after medication is effective are performed surgically and involve a doctor using tools to terminate the pregnancy.
In the politicized discussions around abortion, much has been made about the pain mothers and, or fetus’ feel during abortion. Studies have shown that for pregnant people, abortion is safer than carrying a pregnancy to term and birth. This was also true for most of US history. Pregnancy is not a health-neutral event and carries with it risks–including the risk of death. For the embryo or fetus, abortion ends the lifelike activity, but it is debated by professionals how painful this is and the evidence varies by when the abortion is performed. Public opinion polls have varied since the 1960s on abortion, most people agree it is ending life, but most also feel it’s different from ending the life of something that has been born.
Throughout the early 20th century women and their doctors were put on trial for violating state abortion laws. By 1910, abortion was illegal in every state in the US. Only some states had built in exceptions to save the mother’s life. The decision of when a mother’s life was in jeopardy was left to doctors, who were almost all men, and these standards were not universal.
Making abortion illegal, also known as criminalizing it, simply meant that more women turned away from qualified people to have abortions. Getting abortions under extreme circumstances by people willing to do something illegal, resulted in an increased death toll for mothers. Abortion was not inherently unsafe, illegal abortion was. In 1930, nearly 2,700 US women died from an illegal abortion, or one in five maternal deaths that year.
Doctors caught performing abortions were put on trial and lost their medical licenses. Increasingly the press covered stories about women who had died from an illegal abortion. Women’s bodies were found in barrels, chopped up in suitcases, all after a botched abortion by someone unqualified. People began calling for abortion law reform.
But more importantly, women began appearing in court to give testimony as to why they wanted one in the first place. Abortion was so stigmatized that women never talked about it. Stories of safe, successful abortions were never in the press; however, stories about illegal abortions that resulted in death sold papers. Thus, the effect of criminalization was that women who were accused were forced to talk about it publicly. Women who believed they would never get an abortion listened to abortion stories and empathized with the mothers choice, given her circumstances. Criminalization forced women to talk about their darkest moments in a very public forum.
In 1955, Planned Parenthood called for a national conference on abortion. The few doctors who attended called for greater flexibility for doctors to perform abortions. These doctors had personally witnessed women dying from pregnancy-related causes unable to help them, or watched women carry babies to term knowing the baby could not survive more than a week or so.
Then in the 1960s a drug often prescribed to women to treat pregnancy discomforts, like morning sickness, was found to cause birth defects in babies. A television personality, Sherri Chessen Finkbine was expecting her fifth child when she consumed tranquilizers that her husband brought from England to relieve her nausea, the drug thalidomide. However, after reading an article about thalidomide that discussed its role in the birth of thousands of babies born without arms or legs, Finkbine became worried about the potential harm to her unborn child. Finkbine's doctor confirmed her fears, but at the time, there was no test to assess the fetus's condition. So, following her doctor's suggestion, Finkbine and her husband decided to quietly have an abortion. Abortion in Arizona was illegal, so they ended up traveling to Sweden. Her case was public and public opinion polls showed that 52% of Americans supported her choice under the circumstances.
Ironically, the United States did not witness a pharmaceutical disaster on par with Europe related to Thalidomide because of one scientist at the Food and Drug Administration (FDA): Dr. Frances Kathleen Oldham Kelsey. Dr. Kelsey worked for the American Medical Association and eventually taught pharmacology at the University of South Dakota. In addition to her Ph.D., she also had her medical degree and briefly worked as general practitioner. It was in her first month in her position at the FDA that Dr. Kelsey was taked with evaluating the drug thalidomide for approval in the United States. When the manufacturers of thalidomide submitted their information to Dr. Kelsey, she didn’t believe they had provided adequate data to show its safety and asked them to resubmit their application once they had effectively proved its safety. The manufacturers were frustrated by this woman’s attempt to slow their approval process for a drug that was already in widespread use in Europe. Instead of conducting the new tests and submitting a new report, the manufacturers attempted to pressure and coerce Dr. Kelsey into approval. However, she held firm–trusting her extensive expertise. This back-and-forth is what ultimately caused enough of a delay for word to spread of fetal anomalies and defects in Europe related to thalidomide use by pregnant women. After a congressional hearing on the matter, Dr. Kelsey was able to ensure that thalidomide would be banned in the United States. In 1962, just a year later, President John F. Kennedy granted Dr. Kelsey the President's Award for Distinguished Federal Civilian Service. She was only the second woman to ever receive the award. Kennedy acknowledged "Her exceptional judgment in evaluating a new drug for safety for human use…” In the immediate aftermath of the thalidomide disaster, Dr. Kelsey helped change laws about drug approval to protect the patient, ensure informed consent in clinical trials, and reporting of adverse side effects to the FDA. In her long and distinguished career at the FDA, Dr. Kelsey would eventually become chief of the Division of New Drugs, director of the Division of Scientific Investigations, and deputy for Scientific and Medical Affairs in the Office of Compliance. She retired in 2005, at the age of 90, after 45 years of service.
Dr. Kelsey receiving the President’s Award for Distinguished Federal Civilian Service from President Kennedy. National Library of Medicine, Images from the History of Medicine.
While thousands of babies would be born with thalidomide-related deformities, the United States was spared from a tragedy of that scale. However, when combined with the realization that many of these women in Europe were married and otherwise respectable women and mothers, this public concern about disabled babies–in an era when disability was considered shameful–helped to open the door for discussions about elective abortion and relaxing existing abortion laws.
Despite the stereotype of the young, naive, and sexually promiscuous girl being the ones who get abortions, studies showed that women who were already mothers were more likely to get abortions and that religiosity was not a factor. Women of all faiths got abortions.
In 1964, abortion law reform activists registered their first national group: the Association for the Study of Abortion (ASA). Then in 1966, a group of nine highly regarded California doctors faced a lawsuit for providing abortions to women who had contracted rubella, a disease that could harm unborn babies. However, doctors from all over the country rallied to support these doctors, with even 128 medical school deans joining their defense. As a result, one of the earliest changes to abortion laws in the United States occurred. California revised its strict ban on abortion to permit hospital committees to review and approve requests for the procedure.
Studies in the 1960s showed that poor women and their families were affected to a greater extent from abortion bans. One study examined low-income women in New York City and found that 8% had tried to end a pregnancy through illegal means. Additionally, 38% reported that someone they knew had attempted to get an abortion. Among the low-income women who admitted having an abortion, 77% said they had attempted a self-induced procedure, while only a small fraction 2% involved a medical professional at all.
By the end of the 1960s there was a full fledged movement to repeal abortion bans. National Association for the Repeal of Abortion Laws (NARAL) was founded in 1969. NARAL became the first nationwide organization dedicated exclusively to advocating for the legalization of abortion. Left and right states were repealing or modifying their abortion stances. Alaska, Hawaii, New York, and Washington completely eliminated their laws prohibiting abortion, while 13 other states introduced changes that broadened the circumstances under which abortion was permitted. Instead of solely permitting abortion to save the life of the mother, these reforms allowed for abortion in situations where the pregnancy posed risks to the patient's physical or mental health, when there were fetal abnormalities, or when the pregnancy resulted from rape or incest. However, much of these changes were piecemeal and state by state. It would not be until 1973 that the question of abortion was answered federally.
The Roe v. Wade decision was a landmark ruling by the United States Supreme Court in 1973 that legalized abortion across the country. The case originated in Texas and involved a woman named Norma McCorvey, referred to as "Jane Roe" to protect her identity, who sought to terminate her pregnancy but was denied access to legal abortion under Texas law. In 1969, when McCorvey became pregnant, she was unmarried, financially struggling, and unable to afford to travel to a state where abortion was legal. This also wasn’t her first pregnancy. Texas law at the time prohibited abortion except to save the life of the mother or in instances of rape. McCorvey's lawyers, Linda Coffee and Sarah Weddington, sought a representative plaintiff who could best illustrate the difficulties faced by women seeking abortions. They aimed to demonstrate that the Texas law violated women's constitutional right to privacy. McCorvey's circumstances and her inability to access a safe and legal abortion made her a suitable candidate for the case.
|
|
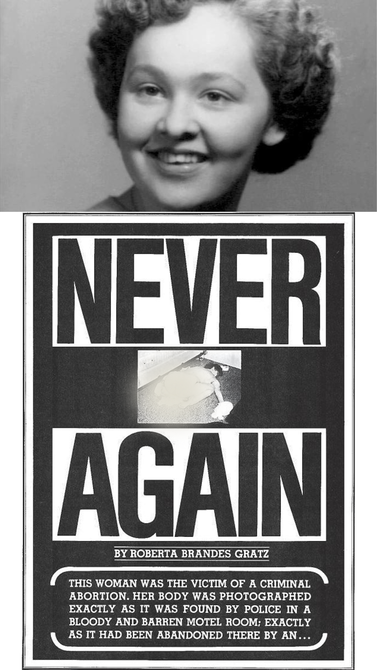 Gerri Santoro in life over the Ms. Magazine cover from 1972 with heading, "Never Again," Public Domain
Gerri Santoro in life over the Ms. Magazine cover from 1972 with heading, "Never Again," Public Domain
Ultimately, building on Griswold v. Connecticut, the Supreme Court, in a 7-2 decision, held that a woman's constitutional right to privacy, as protected by the 14th Amendment, includes the right to choose whether to have an abortion. The Court recognized that this right is not absolute and must be balanced against the government's interest in protecting the potential life of the fetus. It established a framework based on testimony from doctors using the trimesters of pregnancy to determine when and how states could regulate abortion.
In the first trimester, the Court held that the decision to have an abortion should be solely between a woman and her doctor, with minimal government interference. Since the fetus was not viable and legal abortion in the first trimester posed few medical risks, the government’s right to regulate was limited. In the second trimester, the state has a legitimate interest in protecting the woman's health and may regulate abortion to some degree–particularly since second trimester abortions were more dangerous than first trimester abortions, and the fetus was approaching viability. Later court decisions would indicate that these regulations should not impose an "undue burden" on a woman's right to access abortion. In the third trimester, the state's interest in protecting potential life becomes more compelling, and it may prohibit abortion except when necessary to protect the woman's life or health. With the court’s decision in Roe v. Wade, the federal government granted women a right to bodily autonomy, to make their own decisions in family planning, and to engage in sexual relations with the same freedom as men.
It's worth noting that McCorvey never had an abortion during the legal proceedings. By the time the Supreme Court ruled in 1973, she had given birth and placed her child up for adoption.
After the legalization of abortion nationwide, Ms. Magazine, a feminist publication, ran a picture of Gerri Santoro, a young mother who died when her boyfriend tried to perform an abortion on her in a motel room, on their cover. Santoro’s ex-husband was abusive. She fled from him with their children and started a new relationship; however, she never actually divorced her husband. Soon after learning she was pregnant with her boyfriend’s child, her estranged husband contacted her to let her know he would be visiting to see their children. Santoro was terrified he would kill her if he found out she was pregnant with another man’s child, or that he would use her pregnancy with another man in order to take their children away. She and her boyfriend tried to do the abortion themselves, borrowing a medical textbook from the local library. When she began hemorrhaging blood, her boyfriend fled the scene. Ms. Magazine hoped that by telling Santoro’s story people would see how illegal abortion impacted individual women’s lives.
In 1976, the Congress passed the Hyde Amendment to prevent federal funds from being used to support abortions. The funds came from medicaid, a government sponsored insurance program that helps low income families. Women who receive medicaid could not use that insurance to get an abortion. This restriction is still in place today and primarily affects the poor, Black, Latino, and LGBTQ+ communities that predominantly use Medicaid. Women in these categories then are faced with barriers to getting abortions that their wealthier sisters do not. Reproductive Freedom is only possible if the financial and social barriers to freedoms are removed.
In the first trimester, the Court held that the decision to have an abortion should be solely between a woman and her doctor, with minimal government interference. Since the fetus was not viable and legal abortion in the first trimester posed few medical risks, the government’s right to regulate was limited. In the second trimester, the state has a legitimate interest in protecting the woman's health and may regulate abortion to some degree–particularly since second trimester abortions were more dangerous than first trimester abortions, and the fetus was approaching viability. Later court decisions would indicate that these regulations should not impose an "undue burden" on a woman's right to access abortion. In the third trimester, the state's interest in protecting potential life becomes more compelling, and it may prohibit abortion except when necessary to protect the woman's life or health. With the court’s decision in Roe v. Wade, the federal government granted women a right to bodily autonomy, to make their own decisions in family planning, and to engage in sexual relations with the same freedom as men.
It's worth noting that McCorvey never had an abortion during the legal proceedings. By the time the Supreme Court ruled in 1973, she had given birth and placed her child up for adoption.
After the legalization of abortion nationwide, Ms. Magazine, a feminist publication, ran a picture of Gerri Santoro, a young mother who died when her boyfriend tried to perform an abortion on her in a motel room, on their cover. Santoro’s ex-husband was abusive. She fled from him with their children and started a new relationship; however, she never actually divorced her husband. Soon after learning she was pregnant with her boyfriend’s child, her estranged husband contacted her to let her know he would be visiting to see their children. Santoro was terrified he would kill her if he found out she was pregnant with another man’s child, or that he would use her pregnancy with another man in order to take their children away. She and her boyfriend tried to do the abortion themselves, borrowing a medical textbook from the local library. When she began hemorrhaging blood, her boyfriend fled the scene. Ms. Magazine hoped that by telling Santoro’s story people would see how illegal abortion impacted individual women’s lives.
In 1976, the Congress passed the Hyde Amendment to prevent federal funds from being used to support abortions. The funds came from medicaid, a government sponsored insurance program that helps low income families. Women who receive medicaid could not use that insurance to get an abortion. This restriction is still in place today and primarily affects the poor, Black, Latino, and LGBTQ+ communities that predominantly use Medicaid. Women in these categories then are faced with barriers to getting abortions that their wealthier sisters do not. Reproductive Freedom is only possible if the financial and social barriers to freedoms are removed.
 Fannie Lou Hammer, Public Domain
Fannie Lou Hammer, Public Domain
Madrigal v. Quilligan:
A key tenant to Reproductive Justice is the idea of consent, which continued to be a problem through the second half of the 20th century. Family planning initiatives tied to economic policies to end poverty, known as the War on Poverty, funded non-consensual sterilizations of primarily Black and brown women in the 1960s and 1970s.
Fannie Lou Hamer, for example, was an activist and a critically important part of the Civil Rights Movement in the 1960s. She was a leading organizer of the Student Non-Violent Coordinating Committee (SNCC) which played an important role in voter registration drives. She was often one of the only women at the protests.
Earlier in her life, Hamer had seen a physician in Mississippi for removal of a uterine tumor. This was a minor procedure, but Hamer left the hospital only to find out the doctor had also sterilized her without her consent. Hamer later stated, “[In] the North Sunflower County Hospital,...about six out of the 10 Negro women that go to the hospital are sterilized with the tubes tied.”
Some women were sterilized during Cesarean sections and never told, others were threatened with termination of welfare benefits or denial of medical care if they didn’t “consent” to the procedure, others received unnecessary hysterectomies (the surgical removal of the uterus) at teaching hospitals as practice for medical residents. In the South it was such a widespread practice that it had a euphemism: a “Mississippi appendectomy.”
Madrigal v. Quilligan was a class action lawsuit brought on by 10 Latina women in 1978 who represented more than 140 others. These women argued that physicians at the Los Angeles County General Hospital coerced them in the middle of childbirth to consent to surgical sterilization. In some instances, the women were deliberately lied to and told they were consenting to C-sections; in other instances, the women agreed to the surgical sterilizations because they were told they’d die if they got pregnant again, or that the doctors would not assist with childbirth unless they agreed. Some women were presented with consent forms in English, even if the woman signing only had a working understanding of Spanish. In the most extreme instances, the women were not told they had this procedure done at all. They only found out later when they were trying to conceive again.
The Madrigal case illustrates a convergence of the intersections of sex, gender, citizenship, language and culture. Even though the plaintiffs presented a compelling case, a judge ruled in favor of the physicians stating “the staff of a busy metropolitan hospital” had no way of knowing about these women’s “atypical cultural traits.”
In the Madrigal case, it was clear race and sexuality were central to making these women subordinated persons. In the context of the era, many white feminists were calling for access to birth control while minority women were calling for personhood: two very different focus points. For the most part, people of color and their parenting abilities were judged against standards based on white, middle class families. And often, they were found short or lacking by medical professionals and social workers.
A key tenant to Reproductive Justice is the idea of consent, which continued to be a problem through the second half of the 20th century. Family planning initiatives tied to economic policies to end poverty, known as the War on Poverty, funded non-consensual sterilizations of primarily Black and brown women in the 1960s and 1970s.
Fannie Lou Hamer, for example, was an activist and a critically important part of the Civil Rights Movement in the 1960s. She was a leading organizer of the Student Non-Violent Coordinating Committee (SNCC) which played an important role in voter registration drives. She was often one of the only women at the protests.
Earlier in her life, Hamer had seen a physician in Mississippi for removal of a uterine tumor. This was a minor procedure, but Hamer left the hospital only to find out the doctor had also sterilized her without her consent. Hamer later stated, “[In] the North Sunflower County Hospital,...about six out of the 10 Negro women that go to the hospital are sterilized with the tubes tied.”
Some women were sterilized during Cesarean sections and never told, others were threatened with termination of welfare benefits or denial of medical care if they didn’t “consent” to the procedure, others received unnecessary hysterectomies (the surgical removal of the uterus) at teaching hospitals as practice for medical residents. In the South it was such a widespread practice that it had a euphemism: a “Mississippi appendectomy.”
Madrigal v. Quilligan was a class action lawsuit brought on by 10 Latina women in 1978 who represented more than 140 others. These women argued that physicians at the Los Angeles County General Hospital coerced them in the middle of childbirth to consent to surgical sterilization. In some instances, the women were deliberately lied to and told they were consenting to C-sections; in other instances, the women agreed to the surgical sterilizations because they were told they’d die if they got pregnant again, or that the doctors would not assist with childbirth unless they agreed. Some women were presented with consent forms in English, even if the woman signing only had a working understanding of Spanish. In the most extreme instances, the women were not told they had this procedure done at all. They only found out later when they were trying to conceive again.
The Madrigal case illustrates a convergence of the intersections of sex, gender, citizenship, language and culture. Even though the plaintiffs presented a compelling case, a judge ruled in favor of the physicians stating “the staff of a busy metropolitan hospital” had no way of knowing about these women’s “atypical cultural traits.”
In the Madrigal case, it was clear race and sexuality were central to making these women subordinated persons. In the context of the era, many white feminists were calling for access to birth control while minority women were calling for personhood: two very different focus points. For the most part, people of color and their parenting abilities were judged against standards based on white, middle class families. And often, they were found short or lacking by medical professionals and social workers.
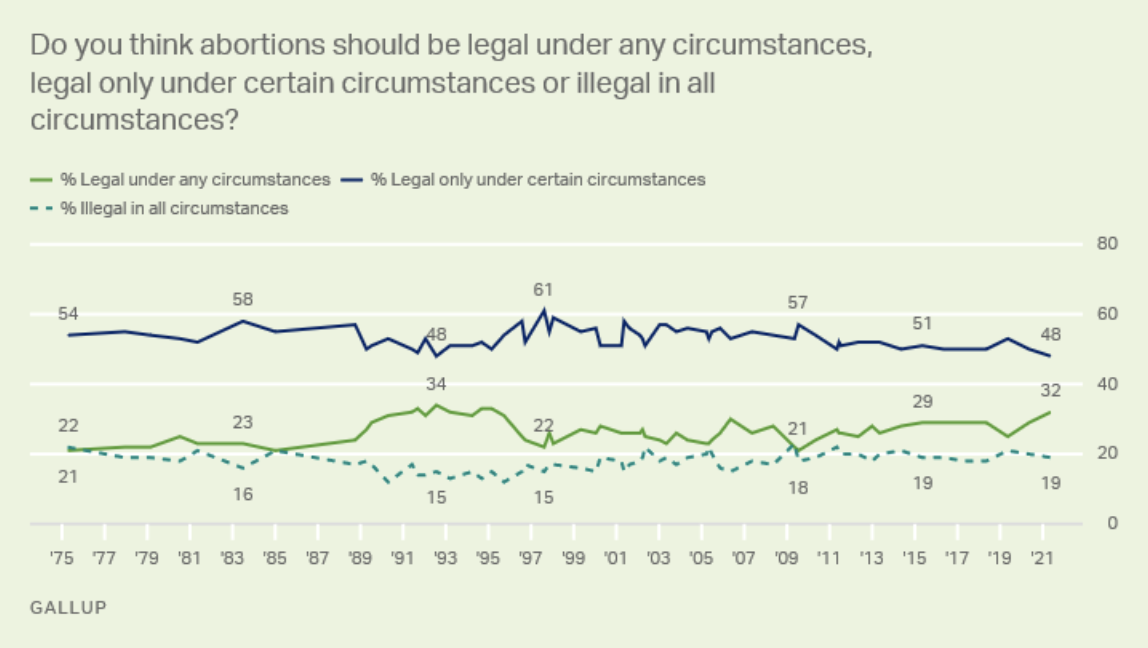
Gallup Polls showing American opinions on the legality of abortion over time.
|
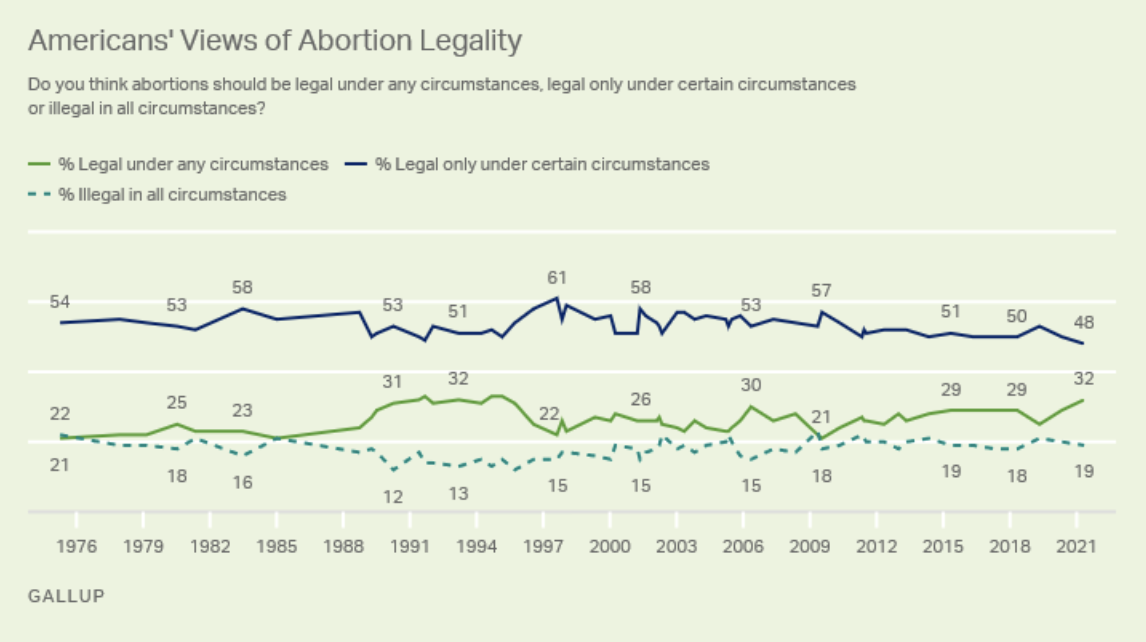
Gallup Polls showing American opinions on the legality of abortion over time.
|
 Silent Scream, Public Domain
Silent Scream, Public Domain
Conservative Opposition:
Many people, women included, opposed and remained opposed to abortion. In 1980, at the end of an era of massive change related to civil and human right enhancements, social shifts gave rise to conservative opposition.
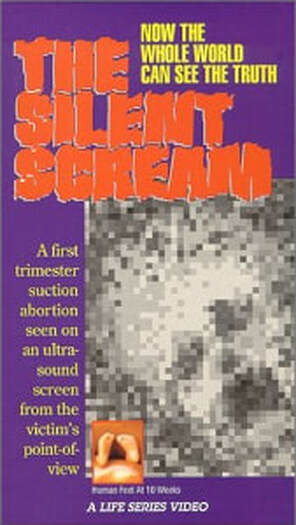
That year anti-abortion activists released a very persuasive propaganda film called Silent Scream. It was a 28-minute long “documentary” of abortion using ultrasound imaging to try and persuade viewers of the wrongs of abortion. It is narrated by an authoritative male voice who claims, "The child," a word chosen to evoke emotion and convey the humanness of the fetus, "senses aggression in its sanctuary" and "agitated" flees from the abortionist’s tools in a "pathetic attempt to escape." The imaging is grainy, but it shows a fetus’ mouth wide open in what the narrator claimed was a "silent scream." This video was altered in a way to support the narrative that abortion was murder.
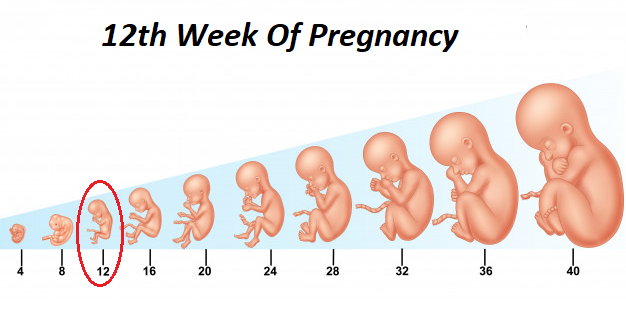
The video editors adjusted the speed of the video to make it appear like the fetus was thrashing about in pain. Doctors who reviewed the film claimed it was deceptive and argued it used special effects. The editors also showed images of an almost full-term baby but claimed it was 12-weeks old. In reality at 12-weeks old, the mother would not be noticeably pregnant, the fetus would be less than 2 inches long, and the fetus would only just recently have begun to resemble a human form.
Although intentionally altered and misleading, the film was weaponized for political means. Reverend Jerry Falwell, a Baptist pastor, televangelist, and conservative activist who founded the political organization known as the Moral Majority, stated that this film “may win the battle for us." The newly elected Republican President, Ronald Reagan supported the film and hoped every member of Congress would view it, calling the last decade of Reproductive Freedom a “tragedy." Anti-abortion groups had copies of the film mailed to every Congressional representative in order to persuade them to vote against abortion, or at least in favor of restrictions.
Over the decades, individual states attempted to limit access to abortion by placing restrictions on the procedure. The 1992 case, Planned Parenthood v. Casey represents the culmination of some of these movements. Though the US Supreme Court’s ruling in the case affirmed the right to abortion, it introduced the “undue burden” standard–which gave states leeway in developing barriers to abortion access; however, what is an undue burden for one woman, many not be an undue burden to another. As such, the barriers that proliferated as a result of this case–like with the Hyde Amendment–primarily prevent poor, low income, rural women, and women of color from accessing safe, legal abortions.
Still, conservatives consistently and effectively pushed a narrative that abortion was dangerous, that women regretted their decisions, and that abortion was murder. These points did not hold up against empirical, scientific studies, which consistently showed that women felt relief, not regret or depression after having an abortion. They also showed that most Americans did not view abortion as murder. In fact, in 1983, only 16 percent of Americans thought it should be illegal. Instead, a large majority felt abortion should be legal: 83% in some circumstances and 23% in all circumstances in 1983. These data altered slightly at times moving closer toward “in all circumstances,” than toward “in some circumstances.”
Opponents to abortion have effectively pushed back against abortion in the case of fetal abnormalities or some sort of “problem” with the way the fetus is developing. In some cases, the fetus may be missing crucial organs, or show signs of severe disability. In other cases, parents may not want to take on the difficulty and financial burden of raising a child with disabilities. Polls have shown that public support for abortion related to fetal abnormality varies depending on the circumstances.
Other studies showed that Americans most supported abortion when the mother’s life or health was in danger and were less favorable of abortions when the woman “wasn’t ready” or didn’t want more children. In a 1996 Gallup Poll survey, 38% of Americans viewed abortion as murder and 10% viewed it as murder but “not as bad as killing a person already born.” With all this polling the wording of the question deeply mattered to results. An analyst from Gallup explained, “Asked about the morality of abortion in general, Americans are evenly divided: 42% told Gallup in a May 2001 survey that abortion is morally acceptable while 45% answered that it is morally wrong. Asked whether abortion is murder, slightly differently worded questions have produced slightly different rates of agreement, ranging between 45% and 57%. Questions that ask whether abortion is an "act of murder" tend to produce answers that are slightly lower than those that simply ask whether abortion is murder.”
Hidden beneath all these opinions were assumptions about gender that impact women daily. Women were supposed to love and sacrifice themselves for their children. They were also supposed to want children. The notion that some women might not was counter to social expectations in the US. Of course many women in history never became mothers, but those women were often ostracized, ridiculed, and condemned as “spinsters” or “witches.”
The most important question to ask regarding abortion, is whether women should have the right to get medical advice from their doctors that could improve their health, even if it meant terminating a pregnancy? And, do the unborn have rights the state should protect at the expense of the mother’s rights to her body?
Many people, women included, opposed and remained opposed to abortion. In 1980, at the end of an era of massive change related to civil and human right enhancements, social shifts gave rise to conservative opposition.
That year anti-abortion activists released a very persuasive propaganda film called Silent Scream. It was a 28-minute long “documentary” of abortion using ultrasound imaging to try and persuade viewers of the wrongs of abortion. It is narrated by an authoritative male voice who claims, "The child," a word chosen to evoke emotion and convey the humanness of the fetus, "senses aggression in its sanctuary" and "agitated" flees from the abortionist’s tools in a "pathetic attempt to escape." The imaging is grainy, but it shows a fetus’ mouth wide open in what the narrator claimed was a "silent scream." This video was altered in a way to support the narrative that abortion was murder.
The video editors adjusted the speed of the video to make it appear like the fetus was thrashing about in pain. Doctors who reviewed the film claimed it was deceptive and argued it used special effects. The editors also showed images of an almost full-term baby but claimed it was 12-weeks old. In reality at 12-weeks old, the mother would not be noticeably pregnant, the fetus would be less than 2 inches long, and the fetus would only just recently have begun to resemble a human form.
Although intentionally altered and misleading, the film was weaponized for political means. Reverend Jerry Falwell, a Baptist pastor, televangelist, and conservative activist who founded the political organization known as the Moral Majority, stated that this film “may win the battle for us." The newly elected Republican President, Ronald Reagan supported the film and hoped every member of Congress would view it, calling the last decade of Reproductive Freedom a “tragedy." Anti-abortion groups had copies of the film mailed to every Congressional representative in order to persuade them to vote against abortion, or at least in favor of restrictions.
Over the decades, individual states attempted to limit access to abortion by placing restrictions on the procedure. The 1992 case, Planned Parenthood v. Casey represents the culmination of some of these movements. Though the US Supreme Court’s ruling in the case affirmed the right to abortion, it introduced the “undue burden” standard–which gave states leeway in developing barriers to abortion access; however, what is an undue burden for one woman, many not be an undue burden to another. As such, the barriers that proliferated as a result of this case–like with the Hyde Amendment–primarily prevent poor, low income, rural women, and women of color from accessing safe, legal abortions.
Still, conservatives consistently and effectively pushed a narrative that abortion was dangerous, that women regretted their decisions, and that abortion was murder. These points did not hold up against empirical, scientific studies, which consistently showed that women felt relief, not regret or depression after having an abortion. They also showed that most Americans did not view abortion as murder. In fact, in 1983, only 16 percent of Americans thought it should be illegal. Instead, a large majority felt abortion should be legal: 83% in some circumstances and 23% in all circumstances in 1983. These data altered slightly at times moving closer toward “in all circumstances,” than toward “in some circumstances.”
Opponents to abortion have effectively pushed back against abortion in the case of fetal abnormalities or some sort of “problem” with the way the fetus is developing. In some cases, the fetus may be missing crucial organs, or show signs of severe disability. In other cases, parents may not want to take on the difficulty and financial burden of raising a child with disabilities. Polls have shown that public support for abortion related to fetal abnormality varies depending on the circumstances.
Other studies showed that Americans most supported abortion when the mother’s life or health was in danger and were less favorable of abortions when the woman “wasn’t ready” or didn’t want more children. In a 1996 Gallup Poll survey, 38% of Americans viewed abortion as murder and 10% viewed it as murder but “not as bad as killing a person already born.” With all this polling the wording of the question deeply mattered to results. An analyst from Gallup explained, “Asked about the morality of abortion in general, Americans are evenly divided: 42% told Gallup in a May 2001 survey that abortion is morally acceptable while 45% answered that it is morally wrong. Asked whether abortion is murder, slightly differently worded questions have produced slightly different rates of agreement, ranging between 45% and 57%. Questions that ask whether abortion is an "act of murder" tend to produce answers that are slightly lower than those that simply ask whether abortion is murder.”
Hidden beneath all these opinions were assumptions about gender that impact women daily. Women were supposed to love and sacrifice themselves for their children. They were also supposed to want children. The notion that some women might not was counter to social expectations in the US. Of course many women in history never became mothers, but those women were often ostracized, ridiculed, and condemned as “spinsters” or “witches.”
The most important question to ask regarding abortion, is whether women should have the right to get medical advice from their doctors that could improve their health, even if it meant terminating a pregnancy? And, do the unborn have rights the state should protect at the expense of the mother’s rights to her body?
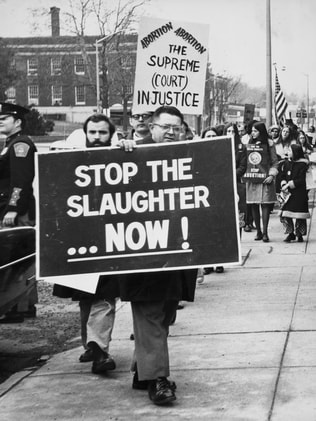 Anti Abortion Protests, Getty Images
Anti Abortion Protests, Getty Images
Conclusion:
Class and race background determined whether women had access to reproductive health care, whether they came into contact with state sterilization and birth control programs, and how they experienced sexuality and reproduction. Over the decades following Roe v. Wade the abortion rate in the country gradually declined after an initial jump, reaching a point lower than when it was entirely illegal by 2017. Experts believe the decline in abortions was due to the availability of reproductive health services, contraceptives, sex education, and other efforts that raised awareness of reproductive freedom. In other words, the less it was stigmatized and the more it was openly discussed, the less abortion was needed or used.
By the end of the 20th century so much about reproductive freedom remained unsettled. Would the court cases survive conservative opposition? Was the basis of these freedoms in the 14th Amendment’s privacy clause strong enough? Although it was legal, would women from diverse backgrounds and poor families be able to access and afford birth control and abortion? Would the stigma of abortion ever go away?
Class and race background determined whether women had access to reproductive health care, whether they came into contact with state sterilization and birth control programs, and how they experienced sexuality and reproduction. Over the decades following Roe v. Wade the abortion rate in the country gradually declined after an initial jump, reaching a point lower than when it was entirely illegal by 2017. Experts believe the decline in abortions was due to the availability of reproductive health services, contraceptives, sex education, and other efforts that raised awareness of reproductive freedom. In other words, the less it was stigmatized and the more it was openly discussed, the less abortion was needed or used.
By the end of the 20th century so much about reproductive freedom remained unsettled. Would the court cases survive conservative opposition? Was the basis of these freedoms in the 14th Amendment’s privacy clause strong enough? Although it was legal, would women from diverse backgrounds and poor families be able to access and afford birth control and abortion? Would the stigma of abortion ever go away?
Draw your own conclusions
|
Learn how to teach with inquiry.
Many of these lesson plans were sponsored in part by the Library of Congress Teaching with Primary Sources Eastern Region Program, coordinated by Waynesburg University, the History and Social Studies Education Faculty at Plymouth State University, and the Patrons of the Remedial Herstory Project. |
|
Lesson Plans from Other Organizations
- The National Women's History Museum has lesson plans on women's history.
- The Guilder Lehrman Institute for American History has lesson plans on women's history.
- The NY Historical Society has articles and classroom activities for teaching women's history.
- Unladylike 2020, in partnership with PBS, has primary sources to explore with students and outstanding videos on women from the Progressive era.
- The Roy Rosenzweig Center for History and New Media has produced recommendations for teaching women's history with primary sources and provided a collection of sources for world history. Check them out!
- The Stanford History Education Group has a number of lesson plans about women in US History.
Period Specific Lesson Plans from Other Organizations
- Clio: In the early 1970s, Boston feminists established a collective to teach themselves and other women about their bodies. Their path-breaking book Our Bodies, Ourselves is now published in 30 languages. In the same era, the Supreme Court ruling Roe v. Wade guaranteed a woman’s right to have an abortion. In the early 1990s, Black women health activists began organizing around the concept of Reproductive Justice, which connects reproductive rights and social justice. Reproductive Justice is defined “as the human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.”
- National History Day: Fannie Lou Hamer (1917-1977) was born Fannie Lou Townsend on October 6, 1917, in Montgomery County, Mississippi. She later moved to Sunflower County where she began sharecropping at the age of six. She married Perry Hammer in 1944 and moved to a plantation in Ruleville, Mississippi. Due to her eighth grade education, she was asked by the plantation owner to serve as the timekeeper, which she did for 18 years. Hamer traveled, unsuccessfully, to Indianola to attempt to vote in 1962. Upon returning to the plantation, she lost her job, forcing her family to find somewhere else to live and work. In 1963, Hamer was named field secretary of the Student Non-violent Coordinating Committee (SNCC). That fall, while traveling back from a training session, she was arrested and brutally beaten in jail. Through her tireless efforts, Hamer was appointed vice-chair of the Mississippi Freedom Democratic Party (MFDP). The following year, the 1965 Voting Rights Act was passed. This pivotal legislation would not have been possible were it not for the efforts of the Mississippi Freedom Democratic Party.
Women and Reproductive Rights
Silent Scream
The voice is assured, unequivocal; the speaker wears a white lab coat, the mantle of medical authority… So begins the film Silent Scream, a 28-minute, shock-the-viewer indictment of abortion. The movie, distributed by American Portrait Films of Anaheim, Calif., depicts through ultrasound imaging what happens in the womb during the abortion of a twelve-week-old fetus. The images are grainy and vague, but Narrator Nathanson provides explanation. "The child," he says, "senses aggression in its sanctuary" and moves in an "agitated" manner away from the surgical instruments in a "pathetic attempt to escape." Its heart rate $ increases as it "senses mortal danger," and, he notes, pointing to a fuzzy image, it opens its mouth in a horrible "silent scream."
The film has been embraced as an effective propaganda weapon by right-to-life organizations. "It may win the battle for us," says the Rev. Jerry Falwell, president of the Moral Majority. In January, even President Reagan gave it high praise. "It's been said that if every member of Congress could see that film," Reagan declared, "they would move quickly to end the tragedy of abortion." Since then, the movie has in fact been sent to every member of Congress and the Supreme Court. Pro-life organizations are financing its distribution (at $100 a videocassette) to state legislators.
Yet among many doctors--especially Nathanson's fellow obstetricians--the film has provoked an outcry. "The problem is that it is factually misleading and unfair," says Dr. Richard Berkowitz, professor of obstetrics and gynecology at New York City's Mount Sinai Medical Center. Special effects may further the deception, according to Dr. John Hobbins of Yale School of Medicine. Early shots of the fetus seem to be run at a slow speed, but when the abortion instruments are introduced, the film is speeded up, creating the illusion that the fetus is thrashing about in alarm. Actually, says Hobbins, "the fetus appears to be acting in a perfectly normal fashion. It's just technical flimflam." Also misleading is the size of the ultrasound image and the doll- like model used in some scenes to represent the fetus. It gives the impression that the twelve-week-old fetus is as big as a full-term baby, when in fact it is less than 2 in. long.
Finally, experts in fetal development argue that at twelve weeks a fetus cannot move "purposefully," as Nathanson asserts, nor can it perceive danger; the cerebral cortex, which coordinates perception and thought, is not yet developed. As for the silent scream, says Johns Hopkins Neurobiologist David Bodian, doctors have no evidence that a twelve-week-old fetus can feel pain, though "there is a possibility of a reflex movement" in response to stimuli like surgical instruments. Hobbins suggests that the dramatic scream may have been a fetal yawn, because "the fetus spends lots of time with its mouth open." Indeed, he says, the gaping mouth in the blurry film may not have been a mouth at all, but the space between the fetal chin and chest.
On Capitol Hill last week, pro-choice activists were responding with a media campaign of their own. Their weapon: a clip from a CBS Morning News show featuring a panel of five physicians, Hobbins and Berkowitz among them, tearing into the film. Doubtless Silent Scream has given pro-life forces new momentum, says Ron Fitzsimmons, a lobbyist for the National Abortion Rights Action League, and "it has forced us to respond."
Wallis, Claudia and Kenneth W. Banta. “Silent Scream.” Time Magazine. Last modified Monday, Mar. 25, 1985. http://www.time.com/time/magazine/article/0,9171,964142,00.html#ixzz1QdckyNXZ
Questions:
The film has been embraced as an effective propaganda weapon by right-to-life organizations. "It may win the battle for us," says the Rev. Jerry Falwell, president of the Moral Majority. In January, even President Reagan gave it high praise. "It's been said that if every member of Congress could see that film," Reagan declared, "they would move quickly to end the tragedy of abortion." Since then, the movie has in fact been sent to every member of Congress and the Supreme Court. Pro-life organizations are financing its distribution (at $100 a videocassette) to state legislators.
Yet among many doctors--especially Nathanson's fellow obstetricians--the film has provoked an outcry. "The problem is that it is factually misleading and unfair," says Dr. Richard Berkowitz, professor of obstetrics and gynecology at New York City's Mount Sinai Medical Center. Special effects may further the deception, according to Dr. John Hobbins of Yale School of Medicine. Early shots of the fetus seem to be run at a slow speed, but when the abortion instruments are introduced, the film is speeded up, creating the illusion that the fetus is thrashing about in alarm. Actually, says Hobbins, "the fetus appears to be acting in a perfectly normal fashion. It's just technical flimflam." Also misleading is the size of the ultrasound image and the doll- like model used in some scenes to represent the fetus. It gives the impression that the twelve-week-old fetus is as big as a full-term baby, when in fact it is less than 2 in. long.
Finally, experts in fetal development argue that at twelve weeks a fetus cannot move "purposefully," as Nathanson asserts, nor can it perceive danger; the cerebral cortex, which coordinates perception and thought, is not yet developed. As for the silent scream, says Johns Hopkins Neurobiologist David Bodian, doctors have no evidence that a twelve-week-old fetus can feel pain, though "there is a possibility of a reflex movement" in response to stimuli like surgical instruments. Hobbins suggests that the dramatic scream may have been a fetal yawn, because "the fetus spends lots of time with its mouth open." Indeed, he says, the gaping mouth in the blurry film may not have been a mouth at all, but the space between the fetal chin and chest.
On Capitol Hill last week, pro-choice activists were responding with a media campaign of their own. Their weapon: a clip from a CBS Morning News show featuring a panel of five physicians, Hobbins and Berkowitz among them, tearing into the film. Doubtless Silent Scream has given pro-life forces new momentum, says Ron Fitzsimmons, a lobbyist for the National Abortion Rights Action League, and "it has forced us to respond."
Wallis, Claudia and Kenneth W. Banta. “Silent Scream.” Time Magazine. Last modified Monday, Mar. 25, 1985. http://www.time.com/time/magazine/article/0,9171,964142,00.html#ixzz1QdckyNXZ
Questions:
- What kind of source is this? Do you find it reliable?
- Was there any language that you found vague or intentionally misleading?
- What does this film argue?
- Why did the panel refute the arguments?
How a Harrowing Photo of One Woman's Death Became an Iconic Pro-Choice Symbol
In 1973, Ms. magazine published a haunting photo of a woman named Gerri Santoro, who'd died of a back-alley abortion. At the time, no one could have predicted what an impact it would have on the pro-choice movement. People knew of Geraldine "Gerri" Santoro's cause of death—an air embolism caused by a back-alley abortion—before they ever knew her name.
On June 8, 1964, the 28-year-old married woman and her lover, Clyde Dixon, checked into Connecticut's now-closed Norwich Motel with no vacation suitcases or change of clothes for an overnight stay. Instead, she brought a catheter and a textbook. Santoro, six and a half months pregnant, was prepared to let Dixon perform her illegal abortion—that is, until she started hemorrhaging during the process and Dixon panicked, abandoning Santoro to bleed to death on the motel floor.
It wasn't until the next day that a maid discovered Santoro's naked body—her torso collapsed over her kneeling legs, with only blood-soaked sheets between her and the carpet.
Santoro's body was photographed for crime scene documentation at the time; in April 1973, nine years after her death and just half a year after the passing of Roe v. Wade, Ms. magazine published the photo of Santoro. At the time, the body was anonymous to them. "Never Again" was the headline that ran with the story and image, which quickly became an iconic symbol of the pro-choice movement. After the passing of Roe v. Wade, the editors at Ms. thought the struggle was finally over. "At that point, we naively believed that would be the end of the story, and that never again would women be lying on the floor in their own blood in a hotel room because of a botched abortion," says Suzanne Braun Levine, who served as Ms.'s first editor from its founding in 1972 to 1988. "That once the Supreme Court had made that ruling, safe abortions would be available to everyone, everywhere." On the other end of the phone, Levine laughs.
Born on August 16, 1935, Gerri Twerdy grew up with ten brothers and four sisters in an old farmhouse in rural, South Coventry, Connecticut. In the 1995 documentary Leona's Sister Gerri, her family and friends recall memories of her: She climbed trees to avoid the chores she disliked, she and her best friend would sneak out of school to change out of their dress code-mandated dresses and into their jeans when playing hooky, and she always smelled like Juicy Fruit gum.
But when she was just 18 years old, in a rush to get hitched before her best friend, Gerri decided to marry a man she had met four weeks prior at a bus stop. His name was Sam Santoro, and he would go on to father two daughters with Gerri—all of whom would become victims of his physical abuse. So when she met 43-year-old Clyde Dixon, a fellow employee at the Mansfield Training School who ostensibly cared for her, she took him as her lover when Sam was living and working in California. But when Gerri found herself pregnant and Sam, unknowing of everything and with an imminent return to Connecticut to visit Gerri and their daughters, she feared for her safety.
So Gerri, or "Margaret Reynolds" according to the motel ledger, checked in to the motel room with Dixon, only to die alone after Dixon had attempted and failed to abort the fetus with a catheter.
Three days later, Dixon and Milton Ray Morgan, a colleague at Mansfield who helped Dixon access the textbook, would be arrested, and Dixon would be charged with manslaughter and "conspiring to commit an illegal abortion." He would go on to serve one year.
An estimated 1.2 million women in the US resorted to illegal abortions every single year before Roe v. Wade, and those abortions directly led to as many as 5,000 annual deaths, according to the NARAL Foundation. The more restrictive the abortions laws are in a given state or country, the higher the instances of unsafe abortions, which today account for about 13 percent of maternal deaths globally, according to a 2008 World Health Organization study.
"Unsafe abortions are frequently performed by providers lacking qualifications and skills to perform induced abortion, and some abortions are self-induced," the WHO study explains. The lack of safeguards, hygienic conditions, and incorrect administration of medication can lead to things like post-abortion sepsis, hemorrhaging, and genital trauma—all of which can all lead to death.
When the Supreme Court decided 7-2 in Roe v. Wade on January 22, 1973, overruling all state laws that restrict or prohibit a woman's right to obtain an abortion during her first three months of pregnancy, Levine and Roberta Brandes-Gratz, the woman who wrote the accompanying story with the nine-year-old image in Ms., both believed that they had won the fight.
...Today the death rate from induced abortion is 0.6 for every 100,000 procedures in the US, making abortion as safe as an injection of penicillin, according to the WHO. Abortion-related deaths are also "rare in countries where the procedure is legal, accessible, and performed early in pregnancy by skilled providers," according to NARAL.
..."One or two generations of young women don't know the genesis of this photograph," Brandes-Gratz says. "This image that was the consequence of a backwards legal system that turned women not only into criminals, but often into corpses. Who expected, who would've anticipated, how much backtracking would occur since."
Arnold, Amanda. “How a Harrowing Photo of One Woman's Death Became an Iconic Pro-Choice Symbol.” Vice. Last modified October 26, 2016.
Questions:
On June 8, 1964, the 28-year-old married woman and her lover, Clyde Dixon, checked into Connecticut's now-closed Norwich Motel with no vacation suitcases or change of clothes for an overnight stay. Instead, she brought a catheter and a textbook. Santoro, six and a half months pregnant, was prepared to let Dixon perform her illegal abortion—that is, until she started hemorrhaging during the process and Dixon panicked, abandoning Santoro to bleed to death on the motel floor.
It wasn't until the next day that a maid discovered Santoro's naked body—her torso collapsed over her kneeling legs, with only blood-soaked sheets between her and the carpet.
Santoro's body was photographed for crime scene documentation at the time; in April 1973, nine years after her death and just half a year after the passing of Roe v. Wade, Ms. magazine published the photo of Santoro. At the time, the body was anonymous to them. "Never Again" was the headline that ran with the story and image, which quickly became an iconic symbol of the pro-choice movement. After the passing of Roe v. Wade, the editors at Ms. thought the struggle was finally over. "At that point, we naively believed that would be the end of the story, and that never again would women be lying on the floor in their own blood in a hotel room because of a botched abortion," says Suzanne Braun Levine, who served as Ms.'s first editor from its founding in 1972 to 1988. "That once the Supreme Court had made that ruling, safe abortions would be available to everyone, everywhere." On the other end of the phone, Levine laughs.
Born on August 16, 1935, Gerri Twerdy grew up with ten brothers and four sisters in an old farmhouse in rural, South Coventry, Connecticut. In the 1995 documentary Leona's Sister Gerri, her family and friends recall memories of her: She climbed trees to avoid the chores she disliked, she and her best friend would sneak out of school to change out of their dress code-mandated dresses and into their jeans when playing hooky, and she always smelled like Juicy Fruit gum.
But when she was just 18 years old, in a rush to get hitched before her best friend, Gerri decided to marry a man she had met four weeks prior at a bus stop. His name was Sam Santoro, and he would go on to father two daughters with Gerri—all of whom would become victims of his physical abuse. So when she met 43-year-old Clyde Dixon, a fellow employee at the Mansfield Training School who ostensibly cared for her, she took him as her lover when Sam was living and working in California. But when Gerri found herself pregnant and Sam, unknowing of everything and with an imminent return to Connecticut to visit Gerri and their daughters, she feared for her safety.
So Gerri, or "Margaret Reynolds" according to the motel ledger, checked in to the motel room with Dixon, only to die alone after Dixon had attempted and failed to abort the fetus with a catheter.
Three days later, Dixon and Milton Ray Morgan, a colleague at Mansfield who helped Dixon access the textbook, would be arrested, and Dixon would be charged with manslaughter and "conspiring to commit an illegal abortion." He would go on to serve one year.
An estimated 1.2 million women in the US resorted to illegal abortions every single year before Roe v. Wade, and those abortions directly led to as many as 5,000 annual deaths, according to the NARAL Foundation. The more restrictive the abortions laws are in a given state or country, the higher the instances of unsafe abortions, which today account for about 13 percent of maternal deaths globally, according to a 2008 World Health Organization study.
"Unsafe abortions are frequently performed by providers lacking qualifications and skills to perform induced abortion, and some abortions are self-induced," the WHO study explains. The lack of safeguards, hygienic conditions, and incorrect administration of medication can lead to things like post-abortion sepsis, hemorrhaging, and genital trauma—all of which can all lead to death.
When the Supreme Court decided 7-2 in Roe v. Wade on January 22, 1973, overruling all state laws that restrict or prohibit a woman's right to obtain an abortion during her first three months of pregnancy, Levine and Roberta Brandes-Gratz, the woman who wrote the accompanying story with the nine-year-old image in Ms., both believed that they had won the fight.
...Today the death rate from induced abortion is 0.6 for every 100,000 procedures in the US, making abortion as safe as an injection of penicillin, according to the WHO. Abortion-related deaths are also "rare in countries where the procedure is legal, accessible, and performed early in pregnancy by skilled providers," according to NARAL.
..."One or two generations of young women don't know the genesis of this photograph," Brandes-Gratz says. "This image that was the consequence of a backwards legal system that turned women not only into criminals, but often into corpses. Who expected, who would've anticipated, how much backtracking would occur since."
Arnold, Amanda. “How a Harrowing Photo of One Woman's Death Became an Iconic Pro-Choice Symbol.” Vice. Last modified October 26, 2016.
Questions:
- What kind of source is this? Do you find it reliable?
- Was there any language that you found vague or intentionally misleading?
- What was it like before abortion was illegal in the US, according to this document?
Girl Death Quiz Opens

GIRL DEATH QUIZ OPENS
Grand Jury to Investigate “Doctor’s” Activities and Two Men Sought
---
An investigation by the county grand jury of the activities of “Dr.” Harley Heddens in his so-called rest home at 27 West Fifty-fifth street was ordered yesterday as police continued their inquiry of asserted illegal operations
Determination to carry the case before the grand jury came as police sought and asserted chiropractor and a medical supply salesman believed to have acted as “solicitor” for Heddens
Police began their investigation of Heddens’s practices Monday with the death in General Hospital of Ruth Attaway, 16-year-old girl of 1063 South Hicks St., Belvedere. She was asserted to have been a patient of Heddens.
CONFESSION ASSERTED
In connection with the grand jury program, Captain of Detectives Davis of the police homicide squad, announced that Heddens has confessed to illegal practice. Under arrest, with Heddens is his wife, Rose Marie, 25, and her sister and brother, Clara and Theo Fournelle.
Heddens is booked on suspicion of murder as a result of Miss Attaway’s death. His wife and the other couple are held as material witnesses. Harold Dean, 20-year-old asserted sweetheart of the dead girl, is at liberty on $1000 bail on a statutory charge.
MAKES STATEMENT
In the City Hall yesterday Heddens made a long and detailed statement admitting his performed illegal operations on Miss Attaway and two other women. He declared his wife and the Fournelles are not implicated in the matter.
Heddens admitted, police said, that he administered chloroform to his patients and performed the asserted operations without licensed surgical skill or knowledge. He said he had only studied chemistry for two years, and used a method of operation which he learned from an old German doctor years ago.
Hayden said his only equipment in the way of an operating room consisted of a long board laid across the bathtub in the bathroom of his home, Capt. Davis said
He said he was an electrical engineer by vocation and had lived at the 55th street address since last February.
Miss Attaway was taken to head Inns by Dean, captain Davis said, and was subjected to treatment and later moved to Dean's home at 135 E Ave. 35. When she became seriously ill she was removed from there to General Hospital by her mother, miss Jewett Joseph of 1153 1/2 South Indiana Ave.
The girl had previously lived with her divorced father.
Questions:
Grand Jury to Investigate “Doctor’s” Activities and Two Men Sought
---
An investigation by the county grand jury of the activities of “Dr.” Harley Heddens in his so-called rest home at 27 West Fifty-fifth street was ordered yesterday as police continued their inquiry of asserted illegal operations
Determination to carry the case before the grand jury came as police sought and asserted chiropractor and a medical supply salesman believed to have acted as “solicitor” for Heddens
Police began their investigation of Heddens’s practices Monday with the death in General Hospital of Ruth Attaway, 16-year-old girl of 1063 South Hicks St., Belvedere. She was asserted to have been a patient of Heddens.
CONFESSION ASSERTED
In connection with the grand jury program, Captain of Detectives Davis of the police homicide squad, announced that Heddens has confessed to illegal practice. Under arrest, with Heddens is his wife, Rose Marie, 25, and her sister and brother, Clara and Theo Fournelle.
Heddens is booked on suspicion of murder as a result of Miss Attaway’s death. His wife and the other couple are held as material witnesses. Harold Dean, 20-year-old asserted sweetheart of the dead girl, is at liberty on $1000 bail on a statutory charge.
MAKES STATEMENT
In the City Hall yesterday Heddens made a long and detailed statement admitting his performed illegal operations on Miss Attaway and two other women. He declared his wife and the Fournelles are not implicated in the matter.
Heddens admitted, police said, that he administered chloroform to his patients and performed the asserted operations without licensed surgical skill or knowledge. He said he had only studied chemistry for two years, and used a method of operation which he learned from an old German doctor years ago.
Hayden said his only equipment in the way of an operating room consisted of a long board laid across the bathtub in the bathroom of his home, Capt. Davis said
He said he was an electrical engineer by vocation and had lived at the 55th street address since last February.
Miss Attaway was taken to head Inns by Dean, captain Davis said, and was subjected to treatment and later moved to Dean's home at 135 E Ave. 35. When she became seriously ill she was removed from there to General Hospital by her mother, miss Jewett Joseph of 1153 1/2 South Indiana Ave.
The girl had previously lived with her divorced father.
Questions:
- What kind of source is this? Do you find it reliable?
- Can an article about one woman be generalized to represent an era?
- What happened to the woman in this article and what does it tell you about the impact of illegal abortion?
Doctor Cleared in Death Case
Doctor Cleared in Death Case
---
Murder charges against Dr. Earl Eames, Glendale physician and surgeon, who is charged with the death following an asserted illegal operation on 17 year old Louise Dyer, were dismissed yesterday by Municipal Judge Chambers after preliminary hearing.
Eames denied he was in any way responsible for the girl's death.
Questions:
---
Murder charges against Dr. Earl Eames, Glendale physician and surgeon, who is charged with the death following an asserted illegal operation on 17 year old Louise Dyer, were dismissed yesterday by Municipal Judge Chambers after preliminary hearing.
Eames denied he was in any way responsible for the girl's death.
Questions:
- What kind of source is this? Do you find it reliable?
- Can an article about one incident be generalized to represent an era?
- What happened to the doctor in this article and what does it tell you about the impact of illegal abortion on the medical profession?
Boston Daily Globe: Woman's Body in Suit Case
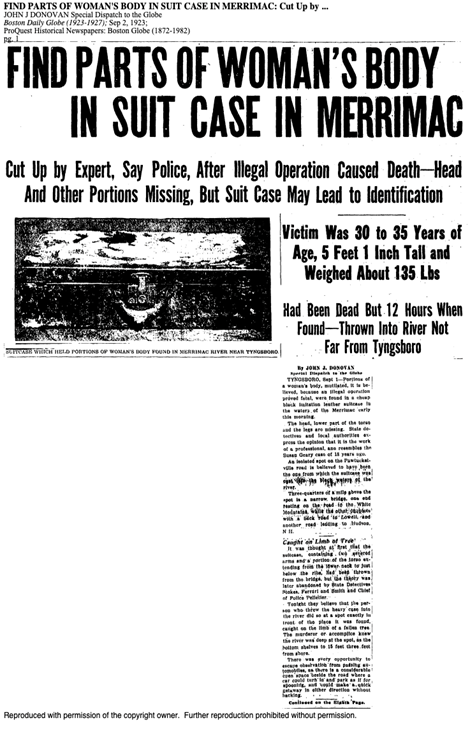
FIND PARTS OF WOMAN’S BODY IN SUIT CASE IN MERRIMAC
Cut Up by Expert, Say Police, After Illegal Operation Caused Death—Head And Other Portions Missing, But Suitcase May Lead to Identification
Victim Was 30 to 35 Years Of Age, 5 Feet 1 Inch Tall and Weighed About 135 Lbs.
Has Been Dead But 12 Hours When Found—Thrown Into A River Not Far From Tyngsboro
By John J. Donovan
Special Dispatch to Globe
TYNGSBORO, Sept. 1—Portions of a woman's body, mutilated, it is believed, because an illegal operation proved fatal, were found in a cheap black imitation leather suitcase in the waters of the Merrimac early this morning.
The head, lower part of the torso and the legs are missing. State detectives and local authorities expressed the opinion that it is the work of a professional, and resembles the Susan Geary case of 18 years ago.
An isolated spot on the Pawtucketville road is believed to have been the one from which the suitcase was cast into the black waters of the river.
Three quarters of a mile above the spot is a narrow bridge, [ILLEGIBLE] resting on the road to the White Mountains, while the other [ILLEGIBLE] with a back row to lull, and another road leading to Hudson NH.
Caught on Limb of Tree
It was thought at first that the suitcase, containing twosevered arms and a portion of the torso extending from the lower neck to just below the ribs, had been thrown from the bridge, but the theory was later abandoned by State Detectives Stokes, Ferrarl and Smith and Chief of Police Pelletier.
Tonight they believe that the person who threw the heavy case into the river did so at a spot exactly in front of the place it was found, caught on the limb of a fallen tree. The murderer or accomplice knew the river was deep at the spot, as the bottom shelves to 15 feet three feet from shore.
There was every opportunity to escape observation from passing automobiles, as there is a considerable open space beside the road where a car could turn in and park as if for spooning, and could make a quick getaway in other direction without [?]cking.
Questions:
Cut Up by Expert, Say Police, After Illegal Operation Caused Death—Head And Other Portions Missing, But Suitcase May Lead to Identification
Victim Was 30 to 35 Years Of Age, 5 Feet 1 Inch Tall and Weighed About 135 Lbs.
Has Been Dead But 12 Hours When Found—Thrown Into A River Not Far From Tyngsboro
By John J. Donovan
Special Dispatch to Globe
TYNGSBORO, Sept. 1—Portions of a woman's body, mutilated, it is believed, because an illegal operation proved fatal, were found in a cheap black imitation leather suitcase in the waters of the Merrimac early this morning.
The head, lower part of the torso and the legs are missing. State detectives and local authorities expressed the opinion that it is the work of a professional, and resembles the Susan Geary case of 18 years ago.
An isolated spot on the Pawtucketville road is believed to have been the one from which the suitcase was cast into the black waters of the river.
Three quarters of a mile above the spot is a narrow bridge, [ILLEGIBLE] resting on the road to the White Mountains, while the other [ILLEGIBLE] with a back row to lull, and another road leading to Hudson NH.
Caught on Limb of Tree
It was thought at first that the suitcase, containing twosevered arms and a portion of the torso extending from the lower neck to just below the ribs, had been thrown from the bridge, but the theory was later abandoned by State Detectives Stokes, Ferrarl and Smith and Chief of Police Pelletier.
Tonight they believe that the person who threw the heavy case into the river did so at a spot exactly in front of the place it was found, caught on the limb of a fallen tree. The murderer or accomplice knew the river was deep at the spot, as the bottom shelves to 15 feet three feet from shore.
There was every opportunity to escape observation from passing automobiles, as there is a considerable open space beside the road where a car could turn in and park as if for spooning, and could make a quick getaway in other direction without [?]cking.
Questions:
- What kind of source is this? Do you find it reliable?
- Can an article about one woman be generalized to represent an era?
- What happened to the woman in this article and what does it tell you about the impact of illegal abortion?
Newspaper: Death Laid to Operation

Death Laid to Operation
Coroner’s Jury Names No One, However, In Case of Mother-to-Be
Investigation by a Coroner's jury yesterday into the death of Mrs. Margaret Simon, 35, housewife, resulted in a verdict that the woman died from the effects of an illegal operation and that the operation constituted a criminal act.
Although, after a police investigation instituted at the request of the husband, Arthur [B] Simon, Dr. J. Carl Cummings, of 220 N Central Ave, Glendale, was held on suspicion of murder. On Wednesday his name was not read into the verdict.
Dr. Cummings, who misses Simon assertedly visited prior to her death at the Wilshire Hospital on May 20th, declined to testify yesterday on the advice of his attorney.
HEARING SET JUNE 8
He was released on $5000 bail following arraignment before Police Judge Frank H. Lowe Wednesday, and will have his preliminary hearing before Judge Lowe at 10:00 AM June 8.
Taking the witness stand yesterday, Dr. Paul B McCracken, the Simon’s family physician testified that Mrs. Simmons came to him for an examination on May 1 and that he informed her she was to become a mother.
He was called to see the woman at her home, 5621 1/2 Meridian St. Highland Park, on May 16, Dr. McCracken testified. he said he found her seriously ill and running a high temperature. She was immediately taken to the hospital.
At the hospital Mrs. Simon told him she had been to see doctor Cummings and that the action to thwart childbirth had been taken, Dr. McCracken said.
NURSE TESTIFIES
Miss Matilda Ofstedal, nurse who attended Mrs. Simon at the hospital, testified she was present when the woman told doctor McCracken of her visits to Dr. Cummings.
The husband told the jury he had no knowledge of his wife's visits to Dr. Cummings until shortly before her death.
An autopsy report to the effect that misses Simon died as the result of an illegal obturation made by Dr. Lewis J Gogol deputy county autopsy surgeon was read to the jury.
Dep. DIst. Atty. Charles W Matthews said he will take no action until after Dr.Cummings preliminary hearing.
Questions:
Coroner’s Jury Names No One, However, In Case of Mother-to-Be
Investigation by a Coroner's jury yesterday into the death of Mrs. Margaret Simon, 35, housewife, resulted in a verdict that the woman died from the effects of an illegal operation and that the operation constituted a criminal act.
Although, after a police investigation instituted at the request of the husband, Arthur [B] Simon, Dr. J. Carl Cummings, of 220 N Central Ave, Glendale, was held on suspicion of murder. On Wednesday his name was not read into the verdict.
Dr. Cummings, who misses Simon assertedly visited prior to her death at the Wilshire Hospital on May 20th, declined to testify yesterday on the advice of his attorney.
HEARING SET JUNE 8
He was released on $5000 bail following arraignment before Police Judge Frank H. Lowe Wednesday, and will have his preliminary hearing before Judge Lowe at 10:00 AM June 8.
Taking the witness stand yesterday, Dr. Paul B McCracken, the Simon’s family physician testified that Mrs. Simmons came to him for an examination on May 1 and that he informed her she was to become a mother.
He was called to see the woman at her home, 5621 1/2 Meridian St. Highland Park, on May 16, Dr. McCracken testified. he said he found her seriously ill and running a high temperature. She was immediately taken to the hospital.
At the hospital Mrs. Simon told him she had been to see doctor Cummings and that the action to thwart childbirth had been taken, Dr. McCracken said.
NURSE TESTIFIES
Miss Matilda Ofstedal, nurse who attended Mrs. Simon at the hospital, testified she was present when the woman told doctor McCracken of her visits to Dr. Cummings.
The husband told the jury he had no knowledge of his wife's visits to Dr. Cummings until shortly before her death.
An autopsy report to the effect that misses Simon died as the result of an illegal obturation made by Dr. Lewis J Gogol deputy county autopsy surgeon was read to the jury.
Dep. DIst. Atty. Charles W Matthews said he will take no action until after Dr.Cummings preliminary hearing.
Questions:
- What kind of source is this? Do you find it reliable?
- Can an article about one woman be generalized to represent an era?
- What happened to the woman in this article and what does it tell you about the impact of illegal abortion?
Lesbian Bars
Dr. Marie Cartier: Baby, You Are My Religion
Prior to 1973, as many of you know, gay people were considered the nation’s largest security risk; more of us were let go of our jobs because of McCarthy than because we were homosexual rather than communist. The question was more often are you or have you ever been a homosexual than are you or have you ever been a communist? We were considered mentally ill until 1973, and there was no major or minor religion that considered us anything other than sinners. So to have any place that we could have community was not rare, it was impossible outside of the one public space that was available, which was the gay bar. So… for people pre-Stonewall, the gay bars operated as an alternate church space.
Cartier, Marie. “Dr. Marie Cartier presents ‘Baby You Are My Religion’ at ALMS 2011 Hosted by Mazer.” Keynote Address at ALMS. YouTube. 2011. Retrieved from https://www.youtube.com/watch?v=9kaS_pGyxmg&t=3s.
Cartier, Marie. “Dr. Marie Cartier presents ‘Baby You Are My Religion’ at ALMS 2011 Hosted by Mazer.” Keynote Address at ALMS. YouTube. 2011. Retrieved from https://www.youtube.com/watch?v=9kaS_pGyxmg&t=3s.
Dr. Marie Cartier: Myrna's Story
I came out as gay in 1945, the year that the war ended[…]I was dating a softball player than I met at the gay bar. I met her at Mona's, or as it was the Paper Pony. My first night in a gay bar was freedom. I had a gay male friend and he took me there. Burner was in the gay bars for eight years; She showed me her treasure from the 40s— a gold softball on a necklace chain from her first lover, inscribed with the initials from the professional softball league, to which women belong to, while the men were in the war. We went to the bar all the time. My entire social life was there, there was no other place.[…]I had insomnia— I used to phone up all the gay bars just to hear them answer the phone; just to hear the noise, oh yes. [I would call] just hear [to] the noise and the laughter in the background. I just wanted to be there me.
Cartier, Marie. “Dr. Marie Cartier presents ‘Marie Cartier reads Myrna's Story.” Presented at WeHo Lesbian Speaker Series. YouTube. September 2016. Retrieved from https://www.youtube.com/watch?v=FmURQ0iwhAM&t=5s.
Cartier, Marie. “Dr. Marie Cartier presents ‘Marie Cartier reads Myrna's Story.” Presented at WeHo Lesbian Speaker Series. YouTube. September 2016. Retrieved from https://www.youtube.com/watch?v=FmURQ0iwhAM&t=5s.
Dr. Marie Cartier: Theresa's Story
This woman had separated with her husband and was working as a migratory farmer with her new girlfriend when her ex-husband tracked them down. This is how she described that encounter.
“We went to Beaumont to pick cherries and we made like 50 cents an hour. And yes my ex-husband tracked me down, had a gun. She ran out of the trailer. He hit me in the face with the gun and I still have a scar, but that didn't stop me.”
Anonymous. “Marie Cartier Introduction to Informants for her book Baby, You Are My Religion.” YouTube. June L. Mazer Lesbian Archives. November 3, 2013. https://www.youtube.com/watch?v=EI-yYkKFdx8.
“We went to Beaumont to pick cherries and we made like 50 cents an hour. And yes my ex-husband tracked me down, had a gun. She ran out of the trailer. He hit me in the face with the gun and I still have a scar, but that didn't stop me.”
Anonymous. “Marie Cartier Introduction to Informants for her book Baby, You Are My Religion.” YouTube. June L. Mazer Lesbian Archives. November 3, 2013. https://www.youtube.com/watch?v=EI-yYkKFdx8.
Anonymous: Introduction
“[It] was sort of in a funny place, and [...] it was a nice bar, it was a nice good-looking bar. We had a lot of people, a lot of teachers, a lot of airline hostesses… Barbara had a really good time in the bar. Very religious… I sort of walked out of the convent door in 1967 and more or less walked into the door of a lesbian bar in 1968. They weren't that different— except–except for the lighting. One was stained glass and one with a little grittier. And the first time I ever went to bed with a woman was in the convent. The morning after we woke up and she said to me, something like I don't remember the exact words because it was ‘68 she said, the morning after we done it she said, ‘Wasn't that a remarkable religious experience we had?’ … I knew the difference between being a lesbian and being a nun and that I couldn't stay.”
Anonymous. “Marie Cartier Introduction to Informants for her book Baby, You Are My Religion.” YouTube. June L. Mazer Lesbian Archives. November 3, 2013. https://www.youtube.com/watch?v=EI-yYkKFdx8.
Anonymous. “Marie Cartier Introduction to Informants for her book Baby, You Are My Religion.” YouTube. June L. Mazer Lesbian Archives. November 3, 2013. https://www.youtube.com/watch?v=EI-yYkKFdx8.
Remedial Herstory Editors. "23. REPRODUCTIVE FREEDOM." The Remedial Herstory Project. July 5, 2023. www.remedialherstory.com.
Primary AUTHOR: |
Dr. Alicia Gutierrez-Romine, Dr. Barbara Tischler, Kelsie Brook Eckert
|
Primary ReviewerS: |
Dr. Elizabeth Disney, OBGYN, Jenna Koloski, ML, Katherine Kiefer
|





|
Consulting TeamKelsie Brook Eckert, Project Director
Coordinator of Social Studies Education at Plymouth State University Dr. Barbara Tischler, Consultant Professor of History Hunter College and Columbia University Dr. Alicia Gutierrez-Romine, Consultant Assistant Professor of History at La Sierra University Jacqui Nelson, Consultant Teaching Lecturer of Military History at Plymouth State University Dr. Deanna Beachley Professor of History and Women's Studies at College of Southern Nevada |
EditorsKelsie Brook Eckert
ReviewersColonial
Dr. Margaret Huettl Hannah Dutton Dr. John Krueckeberg 19th Century Dr. Rebecca Noel Michelle Stonis, MA Annabelle L. Blevins Pifer, MA Cony Marquez, PhD Candidate 20th Century Dr. Tanya Roth Dr. Jessica Frazier Mary Bezbatchenko, MA Dr. Alicia Gutierrez-Romine Matthew Cerjak |
In From Back Alley to the Border, Alicia Gutierrez-Romine examines the history of criminal abortion in California and the role abortion providers played in exposing and exploiting the faults in California’s anti-abortion statute throughout the twentieth century. Focused on the patients who used this underground network and the physicians who facilitated it, Gutierrez-Romine provides insight into the world of illegal abortion from the 1920s through the 1960s, including regular physicians as well as women and African American abortionists, and the investigations, scandals, and trials that surrounded them.
How did reproductive justice―defined as the right to have children, to not have children, and to parent―become recognized as a human rights issue? In Reproductive Rights as Human Rights, Zakiya Luna highlights the often-forgotten activism of women of color who are largely responsible for creating what we now know as the modern-day reproductive justice movement.
In Reproductive Justice, sociologist Barbara Gurr provides the first analysis of Native American women’s reproductive healthcare and offers a sustained consideration of the movement for reproductive justice in the United States.
Expanding the social justice discourse surrounding "reproductive rights" to include issues of environmental justice, incarceration, poverty, disability, and more, this crucial anthology explores the practical applications for activist thought on this ever-urgent issue.
|
Tracing the path to the landmark decision in Roe v. Wade and the continuing battle for women's rights, Blumenthal examines, in a straightforward tone, the root causes of the current debate around abortion and repercussions that have affected generations of American women.
Rebecca Todd Peters, a Presbyterian minister and social ethicist, argues that this shaming and judging reflects deep, often unspoken patriarchal and racist assumptions about women and women’s sexual activity. These assumptions are at the heart of what she calls the justification framework, which governs our public debate about abortion, and disrupts our ability to have authentic public discussions about the health and well-being of women and their families.
Author Dr. DeShawn Taylor tells stories of her life, medical training, and practice to center the everyday situations of everyday people struggling with forces outside their control like unaffordable childcare, lack of access to health care, insufficient paid time off, and unsafe communities. She argues that only when we reframe abortion as a social justice issue can we take back the moral high ground from the extremist Christians and “family values” politicians who have controlled the conversation for far too long.
|
Patricia Zavella experienced firsthand the trials and judgments imposed on a working professional mother of color: her own commitment to academia was questioned during her pregnancy, as she was shamed for having children "too young." And when she finally achieved her professorship, she felt out of place as one of the few female faculty members with children. These experiences sparked Zavella’s interest in the movement for reproductive justice. In this book, she draws on five years of ethnographic research to explore collaborations among women of color engaged in reproductive justice activism.
Recognizing the importance of the rights at stake when the law addresses parenting and procreation, the authors in this book re-imagine judicial opinions that address the law's treatment of pregnancy and parenting. The cases cover topics such as forced sterilization, pregnancy discrimination, criminal penalties for women who take illegal drugs while pregnant, and state funding for abortion. Though some of the re-imagined cases come to the same conclusions as the originals, each rewritten opinion analyzes how these cases impact the most vulnerable populations, including people with disabilities, poor women, and women of color.
|
How to teach with Films:
Remember, teachers want the student to be the historian. What do historians do when they watch films?
- Before they watch, ask students to research the director and producers. These are the source of the information. How will their background and experience likely bias this film?
- Also, ask students to consider the context the film was created in. The film may be about history, but it was made recently. What was going on the year the film was made that could bias the film? In particular, how do you think the gains of feminism will impact the portrayal of the female characters?
- As they watch, ask students to research the historical accuracy of the film. What do online sources say about what the film gets right or wrong?
- Afterward, ask students to describe how the female characters were portrayed and what lessons they got from the film.
- Then, ask students to evaluate this film as a learning tool. Was it helpful to better understand this topic? Did the historical inaccuracies make it unhelpful? Make it clear any informed opinion is valid.
Never, Rarely, Sometimes, Always.
|
A pair of teenage girls in rural Pennsylvania travel to New York City to seek out medical help after an unintended pregnancy.
|
|
Bibliography
“Abortion.” Gallup. ND. https://news.gallup.com/poll/1576/abortion.aspx.
Adam, Jamela. “When could women open a bank account?” Forbes Advisor. March 20, 2023. “https://www.forbes.com/advisor/banking/when-could-women-open-a-bank-account/#:~:text=In%201974%2C%20the%20passage%20of,needing%20a%20male%20co%2Dsigner.
ACLU. “Timeline of Important Reproductive Freedom Cases Decided by the Supreme Court.” American Civil Liberties Union. December 1, 2003 https://www.aclu.org/documents/timeline-important-reproductive-freedom-cases-decided-supreme-court.
Brennan, Patricia. “A Private Matter.” Washington Post. June 14, 1992. https://www.washingtonpost.com/archive/lifestyle/tv/1992/06/14/a-private-matter/aa9d8b83-f545-4e1e-b33c-fb860dd0420b/National Park Service Ethnography Program website.
Britannica Editors. “Emma Goldman.” Encyclopedia Britannica. June 23, 2023. https://www.britannica.com/biography/Emma-Goldman.
Collins, Gail, America's Women: Four Hundred Years of Dolls, Drudges, Helpmates, and Heroines. New York, William Morrow, 2003.
DuBois, Ellen Carol, 1947-. Through Women's Eyes : an American History with Documents. Boston :Bedford/St. Martin's, 2005.Indians Editors. “NATIVE AMERICAN WOMEN.” Indians. N.D. http://indians.org/articles/Native-american-women.html.
Frohwirth L, Coleman M, Moore AM. “Managing Religion and Morality Within the Abortion Experience: Qualitative Interviews With Women Obtaining Abortions in the U.S. World Med Health Policy.” 2018;10(4):381-400. doi:10.1002/wmh3.289. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6424365/.
Gold, Rachel Benson. “Lessons from Before Roe: Will Past be Prologue?” Guttmacher Institute. March 2003. https://www.guttmacher.org/gpr/2003/03/lessons-roe-will-past-be-prologue.
“Mental Health Issues and Abortion.” Ibis Reproductive Health, January 9, 2019. https://www.ibisreproductivehealth.org/publications/mental-health-issues-and-abortion.
Nash, Elizabeth and Joerg Dreweke. “The U.S. Abortion Rate Continues to Drop: Once Again, State Abortion Restrictions Are Not the Main Driver.” Guttmacher Institute. Last modified September 18, 2019. https://www.guttmacher.org/gpr/2019/09/us-abortion-rate-continues-drop-once-again-state-abortion-restrictions-are-not-main.
Planned Parenthood. “The Birth Control Pill: A History.” Planned Parenthood. June 2015. https://www.plannedparenthood.org/files/1514/3518/7100/Pill_History_FactSheet.pdf.
Planned Parenthood. “Historical Abortion Law Timeline: 1850 to Today.” Planned Parenthood. N.D. https://www.plannedparenthoodaction.org/issues/abortion/abortion-central-history-reproductive-health-care-america/historical-abortion-law-timeline-1850-today.
Ross, Loretta J. & Rickie Solinger. Reproductive Justice: An Introduction. Berkeley: University of California Press, 2017.
Saad, Lydia. “Public Opinion About Abortion -- An In-Depth Review.” Gallup. Last modified January 22, 2002. https://news.gallup.com/poll/9904/public-opinion-about-abortion-indepth-review.aspx.
Schoen, Johanna. Choice & Coercion: Birth Control, Sterilization, and Abortion in Public Health and Welfare. Chapel Hill: The University of North Carolina Press, 2005.
Stern, Alexandra Minna. “Sterilized in the Name of Public Health: Race, Immigration, and Reproductive Control in Modern California.” American Journal of Public Health 95, no. 7 (July 2005): 1128-1138.
Stern, Alexandra Minna. Eugenic Nation: Faults and Frontiers of Better Breeding in Modern America. Berkeley: University of California Press, 2015.
Szoch, Mary Ed. “The Best Pro-Life Arugments for Secular Audiences.” Center for Human Dignity at Family Research Council. Last modified 2021. https://downloads.frc.org/EF/EF21F56.pdf.
Wade, Lisa. “Sterilization of Women of Color: Does “Unforced” Mean “Freely Chosen”?” Ms. Magazine. July 21, 2011. https://msmagazine.com/2011/07/21/sterilization-of-women-of-color-does-unforced-mean-freely-chosen/.
Ware, Susan. American Women’s History: A Very Short Introduction. Oxford: Oxford University Press, 2015.
Adam, Jamela. “When could women open a bank account?” Forbes Advisor. March 20, 2023. “https://www.forbes.com/advisor/banking/when-could-women-open-a-bank-account/#:~:text=In%201974%2C%20the%20passage%20of,needing%20a%20male%20co%2Dsigner.
ACLU. “Timeline of Important Reproductive Freedom Cases Decided by the Supreme Court.” American Civil Liberties Union. December 1, 2003 https://www.aclu.org/documents/timeline-important-reproductive-freedom-cases-decided-supreme-court.
Brennan, Patricia. “A Private Matter.” Washington Post. June 14, 1992. https://www.washingtonpost.com/archive/lifestyle/tv/1992/06/14/a-private-matter/aa9d8b83-f545-4e1e-b33c-fb860dd0420b/National Park Service Ethnography Program website.
Britannica Editors. “Emma Goldman.” Encyclopedia Britannica. June 23, 2023. https://www.britannica.com/biography/Emma-Goldman.
Collins, Gail, America's Women: Four Hundred Years of Dolls, Drudges, Helpmates, and Heroines. New York, William Morrow, 2003.
DuBois, Ellen Carol, 1947-. Through Women's Eyes : an American History with Documents. Boston :Bedford/St. Martin's, 2005.Indians Editors. “NATIVE AMERICAN WOMEN.” Indians. N.D. http://indians.org/articles/Native-american-women.html.
Frohwirth L, Coleman M, Moore AM. “Managing Religion and Morality Within the Abortion Experience: Qualitative Interviews With Women Obtaining Abortions in the U.S. World Med Health Policy.” 2018;10(4):381-400. doi:10.1002/wmh3.289. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6424365/.
Gold, Rachel Benson. “Lessons from Before Roe: Will Past be Prologue?” Guttmacher Institute. March 2003. https://www.guttmacher.org/gpr/2003/03/lessons-roe-will-past-be-prologue.
“Mental Health Issues and Abortion.” Ibis Reproductive Health, January 9, 2019. https://www.ibisreproductivehealth.org/publications/mental-health-issues-and-abortion.
Nash, Elizabeth and Joerg Dreweke. “The U.S. Abortion Rate Continues to Drop: Once Again, State Abortion Restrictions Are Not the Main Driver.” Guttmacher Institute. Last modified September 18, 2019. https://www.guttmacher.org/gpr/2019/09/us-abortion-rate-continues-drop-once-again-state-abortion-restrictions-are-not-main.
Planned Parenthood. “The Birth Control Pill: A History.” Planned Parenthood. June 2015. https://www.plannedparenthood.org/files/1514/3518/7100/Pill_History_FactSheet.pdf.
Planned Parenthood. “Historical Abortion Law Timeline: 1850 to Today.” Planned Parenthood. N.D. https://www.plannedparenthoodaction.org/issues/abortion/abortion-central-history-reproductive-health-care-america/historical-abortion-law-timeline-1850-today.
Ross, Loretta J. & Rickie Solinger. Reproductive Justice: An Introduction. Berkeley: University of California Press, 2017.
Saad, Lydia. “Public Opinion About Abortion -- An In-Depth Review.” Gallup. Last modified January 22, 2002. https://news.gallup.com/poll/9904/public-opinion-about-abortion-indepth-review.aspx.
Schoen, Johanna. Choice & Coercion: Birth Control, Sterilization, and Abortion in Public Health and Welfare. Chapel Hill: The University of North Carolina Press, 2005.
Stern, Alexandra Minna. “Sterilized in the Name of Public Health: Race, Immigration, and Reproductive Control in Modern California.” American Journal of Public Health 95, no. 7 (July 2005): 1128-1138.
Stern, Alexandra Minna. Eugenic Nation: Faults and Frontiers of Better Breeding in Modern America. Berkeley: University of California Press, 2015.
Szoch, Mary Ed. “The Best Pro-Life Arugments for Secular Audiences.” Center for Human Dignity at Family Research Council. Last modified 2021. https://downloads.frc.org/EF/EF21F56.pdf.
Wade, Lisa. “Sterilization of Women of Color: Does “Unforced” Mean “Freely Chosen”?” Ms. Magazine. July 21, 2011. https://msmagazine.com/2011/07/21/sterilization-of-women-of-color-does-unforced-mean-freely-chosen/.
Ware, Susan. American Women’s History: A Very Short Introduction. Oxford: Oxford University Press, 2015.